Session: PD08: Kidney Cancer: Epidemiology & Evaluation/Staging/Surveillance I
PD08-11: Active Surveillance versus Primary Intervention for Clinical T1a Kidney Tumors: Twelve-Year Experience of the DISSRM Prospective Comparative Study
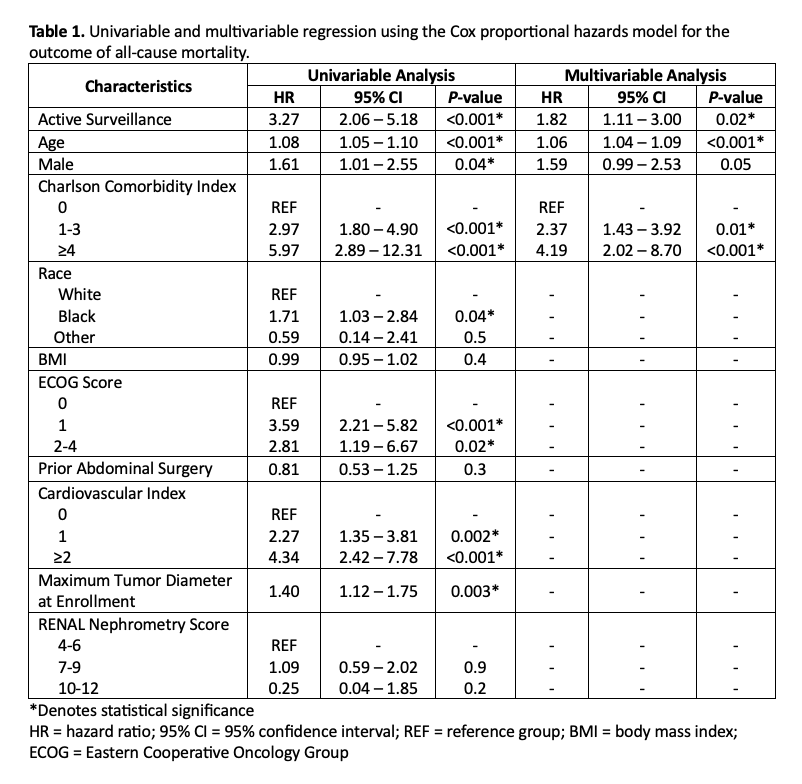
Introduction: Active surveillance (AS) is an alternative to primary intervention (PI) in the management of small renal masses (SRMs; clinical stage T1a). However, AS remains underutilized due to the lack of strong, prospective data. We herein report mature outcomes after a twelve-year experience with the Delayed Intervention and Surveillance for Small Renal Masses (DISSRM) Registry. Methods: the DISSRM Registry has prospectively enrolled patients between 2009 to 2021, this multi-institutional comparative study that includes Johns Hopkins Medical Institution, Beth Israel Deaconess Medical Center, and Columbia University Medical Center. All patients with SRM in the registry chose to either undergo AS or PI. Primary outcomes were cancer-specific survival (CSS) and overall survival (OS); secondary outcomes were progression-free survival (PFS) and recurrence-free survival (RFS). Outcomes were evaluated using Kaplan-Meier survival analysis and log-rank test. Results: A total of 964 patients were enrolled, 785 patients had available follow-up data. Of these 785 patients, 585 (60.68%) chose AS and 379 (39.32%) chose PI. Ultimately, 88 of 585 AS patients (15.04%) crossed over to delayed intervention (DI). Median follow-up time for the registry was 3.39 years (IQR 1.71-6.88), with 331 patients (34.3%) followed for =5 years. There was no difference in CSS between AS and PI (P=0.6). However, AS patients demonstrated worse OS compared to those who underwent PI (P <0.001). In the AS cohort, PFS was 62.1% at 7 years; 76.4% of progressions were due to growth rate >0.5 cm/year. RFS was not different between PI and DI (P=0.7). Unadjusted analysis demonstrated AS was associated with increased all-cause mortality Differences in all-cause mortality between the AS and PI cohorts were attributable to increased age and Charlson Comorbidity Index (CCI)in the AS group (P=0.02). Conclusions: AS is not inferior to PI for carefully selected patients with SRM suspicious for renal cell carcinoma. The difference in OS between AS and PI is mostly attributable to the increased risk of death from competing causes among AS patients. A priori definitions of progression, including growth rate, should be re-considered given high rates of progression with few adverse oncologic outcomes. SOURCE OF Funding: n/a