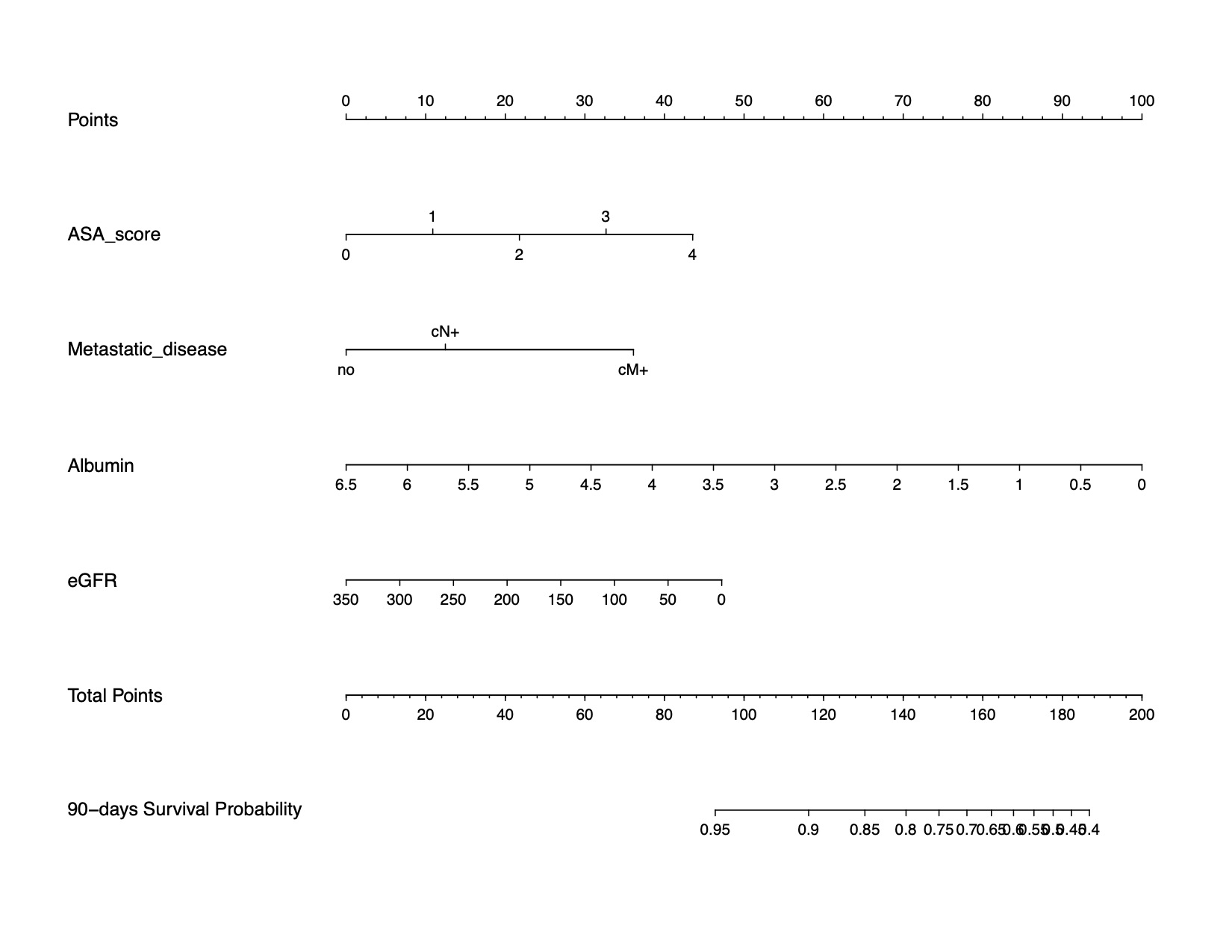
Introduction: Several models for the prediction of 90d mortality after radical cystectomy (RC) based on preoperative parameters have been introduced. This study aimed to externally validate the performance of the existing nomograms and to select the most valuable predictors addressing 90d mortality after RC using a machine-learning-based approach to ultimately help improve outcome prediction in a preoperative setting. Methods: Data of 3,816 bladder cancer patients treated with RC have been retrospectively collected from 25 tertiary referral centers. The abilities of the PROMETRICS2011, Morgan, and Taylor nomograms to predict postoperative 90d mortality were tested. Further, patients were randomly divided into development and validation cohorts. A machine-learning-based variable selection approach (LASSO regression) was used for the fitting of the most informative, yet parsimonious multivariable model to predict 90d mortality after RC. The discriminatory ability of the model was quantified by the area under the curve (AUC) of receiver operating curves (ROC). After validation of the model, a nomogram was created, and decision curve analysis (DCA) was used to evaluate its clinical net-benefit. Results: A total of 269 patients (7%) experienced 90d mortality. During external validation of the existing models in our study population, the PROMETRICS nomogram showed discrimination for predicting individual 90-d mortality with an accuracy of 70.3%. The Morgan and Taylor nomograms showed an accuracy of 67.2% and 61.3%, respectively.Our new model comprised ASA score, clinically metastatic disease, albumin, and eGFR as selected by the machine-learning process to be of high discriminatory power. In the development cohort, the newly developed model had an AUC of 80% whereas the validation cohort showed an AUC of 65%, respectively. In sensitivity analysis including only non-metastatic patients, the AUC addressing 90d mortality after RC was 72%. Conclusions: Our newly developed model for the prediction of 90d mortality after RC outperformed currently available nomograms within a large contemporary cohort. It can be used in a preoperative setting with easily assessable variables for preoperative patient counselling and risk stratification. However, external validation is warranted before clinical use. SOURCE OF Funding: None.