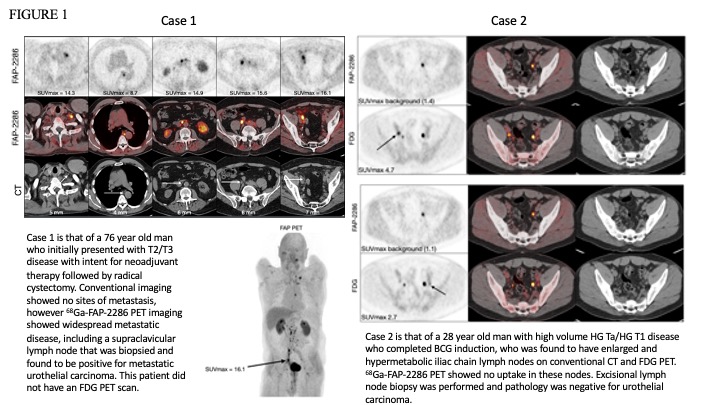
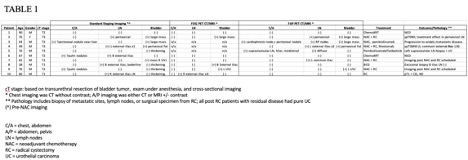
Introduction: Bladder cancer is a common and often aggressive malignancy. Computed tomography (CT), magnetic resonance imaging (MRI) and fluorodeoxyglucose-positron emission tomography (FDG-PET) are used for staging but have limitations in identifying nodal or metastatic disease. Fibroblast activation protein (FAP) is a cell surface protein that is highly expressed on cancer-associated fibroblasts present in many cancers, including bladder cancer. We present the results of a pilot study assessing the diagnostic performance of 68Ga-FAP-2286 (FAP)-PET imaging in a cohort of patients with bladder cancer. Methods: Patients with solid tumors underwent FAP-PET as part of a clinical trial (NCT04621435), including 16 patients with bladder cancer. We report on ten patients with clinically localized disease treated with curative intent at the time of imaging. Standard imaging with CT, MRI, FDG-PET, or bone scan was performed within 8 weeks of FAP-PET. The maximum standardized uptake value (SUV) and size of FAP-PET-positive lesions (defined as any focus of activity with at least 1.5 times higher SUV compared with mediastinal blood pool) were documented. Results: Patient demographics and clinical stage are summarized in Table 1. Concordance of 12 FAP-PET scans was 33% with standard imaging and 43% with FDG-PET. Of 8 patients with pathologic or radiographic follow up, FAP-PET was concordant with true disease status in 100%. Two patients had FAP-PET before and after neoadjuvant chemotherapy; one had resolution of lymph node uptake and one had decreased but persistent uptake on (pathology from pelvic lymph node dissection positive for urothelial carcinoma). We highlight two cases where FAP-PET altered treatment decisions (Figure 1). Conclusions: FAP-PET has the potential to change treatment pathways and improve patient care by better identifying metastatic sites or falsely positive lymph nodes in cancers considered clinically localized and by improving response assessment to systemic therapy. SOURCE OF Funding: IIT from Clovis