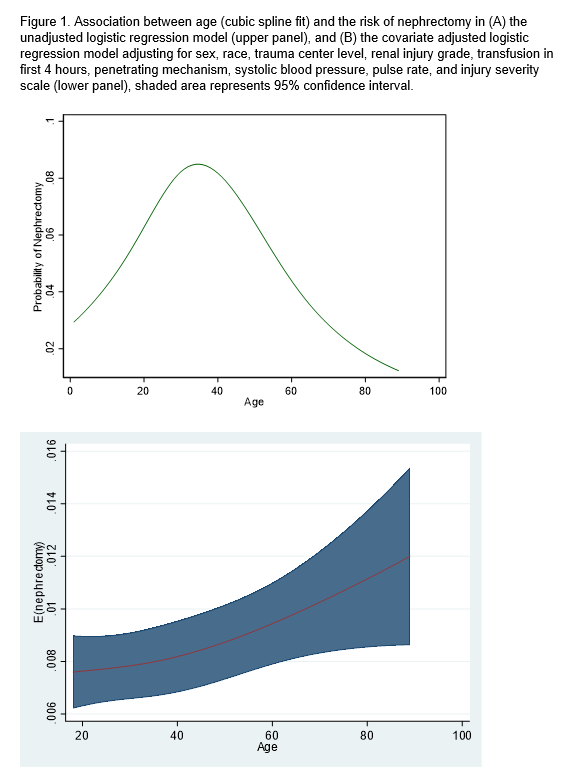
Introduction: More conservative approaches have been utilized for renal trauma management over the last decade. However, certain clinical scenarios warrant further intervention. We sought to determine factors associated with interventions for renal trauma management using contemporary real-world data. Methods: The National Trauma Data Bank (NTDB) was queried for renal trauma with an American Association for the Surgery of Trauma (AAST) grade for patients =18 years old. Patients without AAST grade or with no sign of life were excluded. A logistics regression model was used to determine factors associated with intervention, including nephrectomy, angioembolization, and renorrhaphy. Models were adjusted for patient, hospital, and clinical factors. Results: Our cohort was comprised of 49,884 patients with renal trauma, of which 3,366 (6.8%), 995 (1.9%), and 691 (1.4%) underwent nephrectomy, renorrhaphy, and angioembolization, respectively. Among patients receiving a nephrectomy, patients were more likely to receive a transfusion (OR 3.8, p<0.001), have a penetrating trauma (OR 6.7, p<0.001), have a grade 4 (OR 7.9, p<0.001) or 5 renal trauma (OR 44.7, p<0.001). Patients who had renorrhaphy were more likely to receive a transfusion (OR 1.7, p<0.001) or have a penetrating trauma (OR 44.0, p<0.001). Patients who underwent angioembolization were less likely to be female (OR 0.78, p<0.05), Black (OR 0.71, p<0.01), or have a penetrating trauma (OR 0.31, p<0.001), and were more likely to receive a transfusion (OR 44.8, p<0.001) or have a grade 4 (OR 3.8, p<0.001) or 5 renal trauma (OR 4.2, p<0.001). We observed a complex association between age and probability of nephrectomy. In the unadjusted analysis, there was a peak in nephrectomy for young adults 30-40 years old (Figure 1A). However results of the multivariate model revealed a alternate association where the adjusted risk of nephrectomy was approximately linear and progressively increased with age (Figure 1B). Conclusions: Several patient, hospital, and clinical factors are associated with the use of nephrectomy, renorrhaphy, and angioembolization for the management of renal trauma. These data suggest that older age is an independent predictor of nephrectomy, warranting further research and efforts to improve renal salvage in the elderly population. SOURCE OF Funding: None