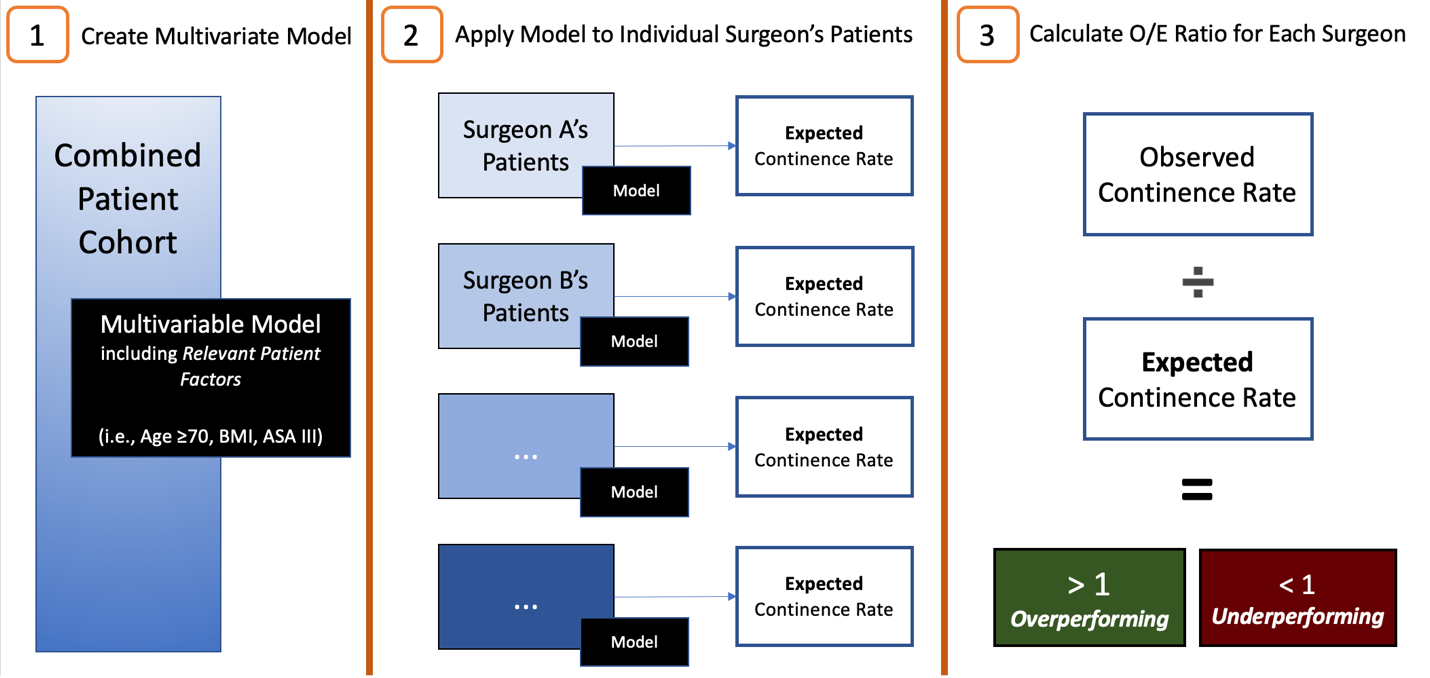
Introduction: Measures of intraoperative performance have supplanted surrogate quality metrics such as surgeon experience. Despite this, evidence supporting the use of surgical skill as a predictor of patient outcomes is often criticized for inadequately controlling for the patient heterogeneity between surgeons’ practices. We use a novel application of case-mix adjustment to demonstrate the robustness of the surgeon skill-to-outcome relationship in robot-assisted radical prostatectomy (RARP). Methods: Bi-institutional, prospectively collected data was analyzed, including demographics, intraoperative video, and postoperative outcomes. The primary outcome was continence recovery (no pads) at 12-months postoperatively. Preoperative clinicopathological factors were evaluated using univariate logistic regression, and variables with a p-value < 0.1 were included in the multivariate model. Surgeons were dichotomized based on observed-to-expected (O/E) ratio, comparing the actual continence rate among their patient with the predicted continence rate based on their patient’s characteristics (Fig 1). Finally, Dissection Assessment for Robotic Technique (DART) scores were provided by 3 independent raters for the nerve-spare (NS) dissection step, and Kruskal-Wallis tests were used to compare scores between surgeon cohorts. Results: Fourteen surgeons contributing a total of 804 cases were included. Patient factors were significantly associated with 12-month continence, including age =70, BMI, and ASA. After applying the multivariate model, seven surgeons were found to have O/E = 1 (i.e., ‘overperforming’). When comparing over- and underperforming surgeons, we did not see significant differences in surgical experience (p=0.38). DART scores across the two groups of surgeons were compared, showing significantly higher Tissue Handling (p=0.002) and Overall dissection skill scores (p=0.003) in the ‘overperforming’ cohort. Conclusions: Surgeon technical skill is predictive of postoperative outcomes, independent of differences in patient characteristics at a surgeon-level. These data add to the robust body of evidence supporting the use of surgical skill as a quality measure, with potential applications across education, accreditation, and patient safety initiatives. SOURCE OF Funding: Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Number R01CA273031. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.