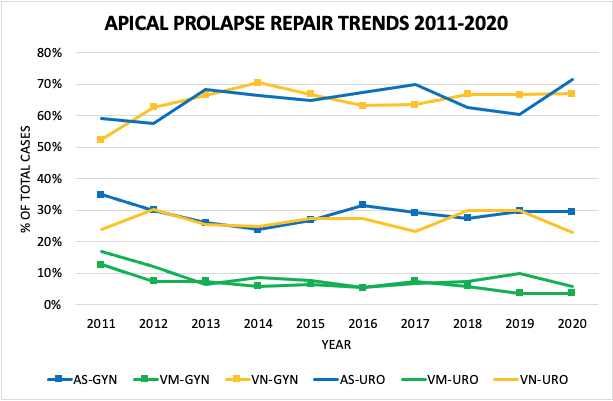
Introduction: Since transvaginal mesh (VM) for apical pelvic organ prolapse (APOP) repair was labeled “high-risk” in 2016 and subsequently banned in 2019 by the US Food and Drug Administration, remaining surgical treatment options include abdominal mesh-augmented sacrocolpopexy (AS) via laparoscopic (LAS) and open (OAS) approaches and vaginal native tissue apical suspension (VN). Our aim was to determine trends in APOP procedures post VM and whether differences existed between urologists and gynecologists. Methods: Between 2011-2020, the National Surgical Quality Improvement Program (NSQIP) database was queried for AS, VM, and VN performed by both urologists and gynecologists. Trends in surgical approach were analyzed. Results: 26,477 cases of APOP repair (32% AS, 6% VM, 62% VN) were included, 9% by urologists. Urologists operated on older (65 vs 61 years) patients with higher ASA score (32% vs 25% ASA III) with a higher prevalence of diabetes, chronic obstructive pulmonary disease, and bleeding disorders (p < 0.05). Mean BMI was 28 and did not vary by specialty. Urologists performed significantly higher proportion of AS (65% vs 29%) and VM (8% vs 6%) relative to VN (27% vs 65%) than gynecologists (p < 0.0001). VM utilization has decreased over time for both urologists (p=0.0242) and gynecologists (p=0.0001); a trend towards increasing AS (p=0.1646) in urologists and VN (p=0.0913) in gynecologists has concurrently occurred. Both specialties have increasingly favored LAS over OAS (p < 0.0001). Operating room times did not vary for AS (p=0.1719) and were slightly higher for urologists in VM (111 vs 106 min, p=0.0432) and VN (118 vs 111 min, p<0.0001). Concurrent mid-urethral mesh sling placement occurred in 29% of cases overall; this has remained unchanged over time for urologists (p=0.8348) and decreased (p=0.0003) for gynecologists. Conclusions: Significant differences in the surgical approach to apical prolapse repair procedures and concomitant mid-urethral mesh slings exist between specialties. Urologists tend to operate on more medically complex and older patients with APOP and continue to demonstrate a strong preference for mesh-augmented repairs compared to transvaginal native tissue repairs. Minimally-invasive sacrocolpopexy is being more frequently performed by both specialties treating APOP. SOURCE OF Funding: None

 photo")