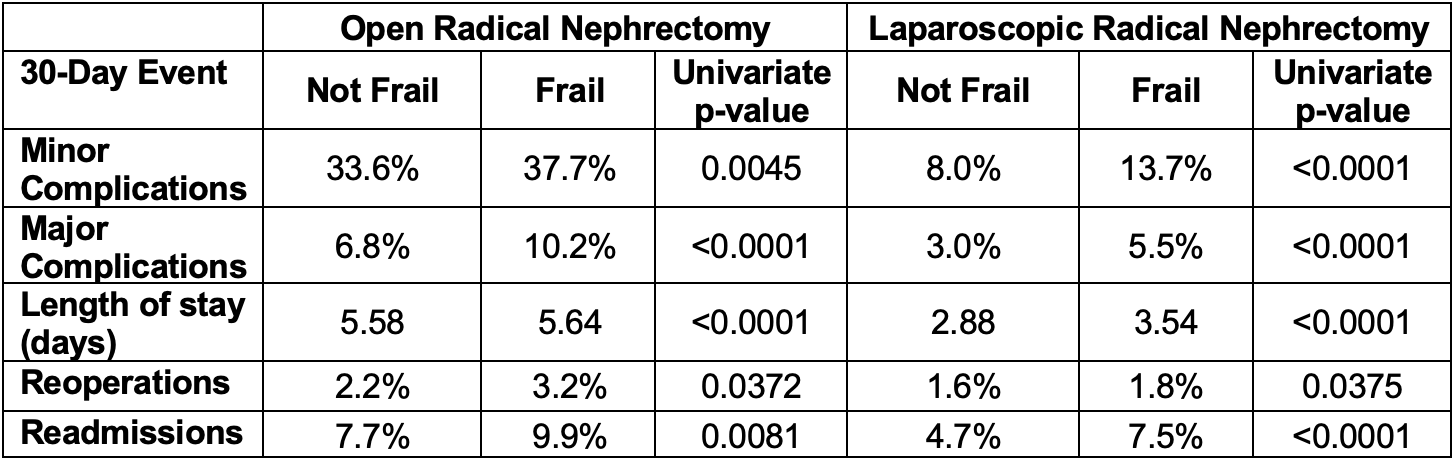
Introduction: As the geriatric population continues to grow, an increasing number of medically frail patients are developing renal masses that necessitate surgical intervention. These patients, however, are significantly more likely to suffer from adverse events following a variety of surgical procedures. We sought to better understand the relationship with frailty and postoperative complications after open (ORN) and laparoscopic (LRN) radical nephrectomy for renal masses. Methods: The National Surgical Quality Improvement Program database was queried for ORN (CPT® 50230) and LRN (CPT® 50545) from 2015-2020. The modified 5-item frailty index (5-MFI) was calculated based on patient functional status and medical comorbidities (diabetes, congestive heart failure, chronic obstructive pulmonary disease, and hypertension requiring medication). Patients with a 5-MFI score =2 were considered medically frail. Associations with 30-day events were analyzed. Results: A total of 6,324 ORN and 15,629 LRN were included, of which 22% and 24%, respectively, were considered frail by at 5-MFI score of =2. Increased age and body mass index (BMI) were significantly associated with frailty for both ORN and LRN (p < 0.05). Upon multivariate analysis controlling for age and BMI in ORN, frailty was independently associated with minor (OR=1.17 [1.03-1.33], p=0.013) and major (OR=1.43 [1.16-1.77], p=0.001) postoperative complications. Both repeat operations (OR=1.56 [1.08-2.25], p=0.018) and readmissions (OR=1.39 [1.12-1.71], p=0.002) were also independently associated with frailty. Similarly for LRN, minor complications (OR=1.75 [1.56-1.98], p<0.001), major complications (OR=1.74 [1.45-2.08], p<0.001) and readmissions (OR=1.62 [1.39-1.90], p<0.001) were independently associated with frailty; reoperations (OR=1.10 [0.82-1.47], p=0.526) were not. Conclusions: Patients considered medically frail are more likely to suffer from 30-day postoperative complications, unplanned readmissions, and reoperations following radical nephrectomy. In the context of an aging population, frailty should be taken into consideration for counseling and postoperative management following radical nephrectomy. SOURCE OF Funding: N/A

 photo")