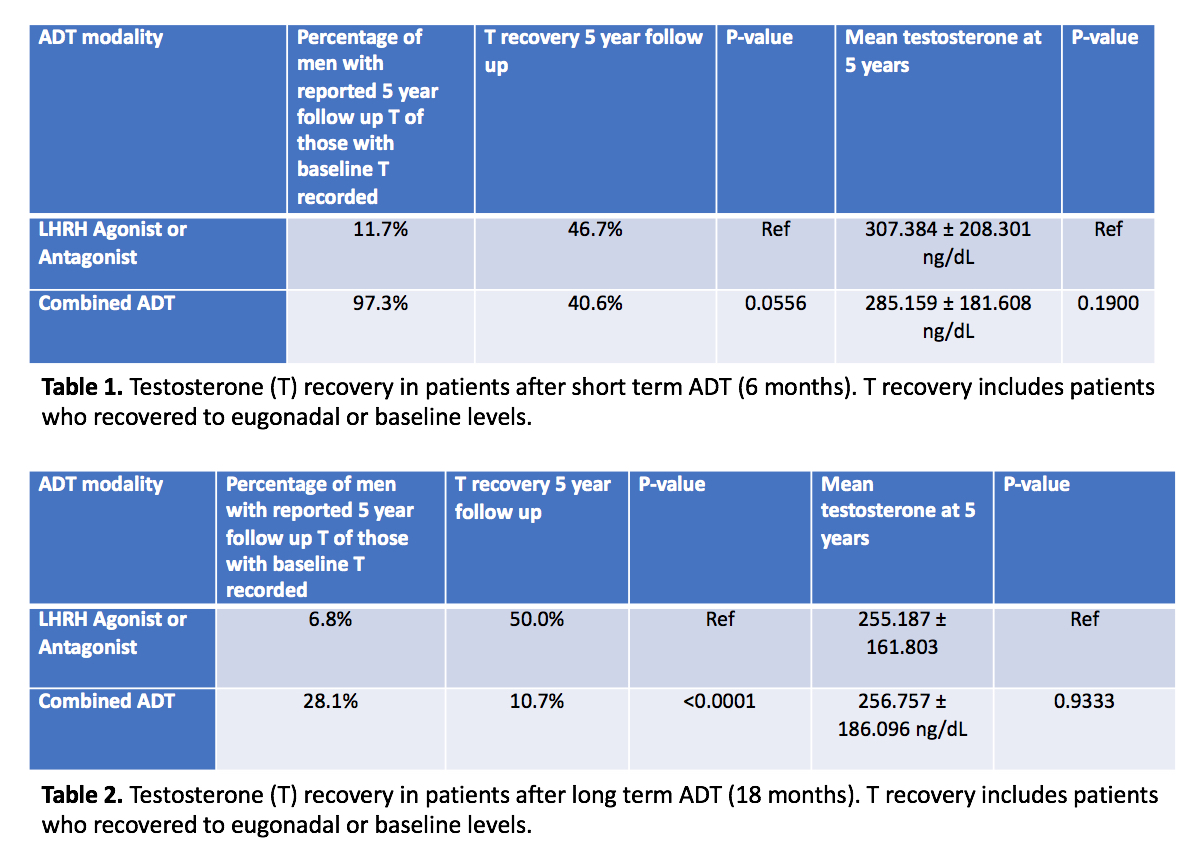
Introduction: Androgen deprivation therapy (ADT) is frequently used in the treatment of localized PCa. Many men receiving temporary ADT for localized prostate cancer fail to achieve baseline testosterone (T) levels after cessation. However, current literature limits the ability to predict prolonged testosterone deficiency (TD) based on ADT regimen and duration. Testosterone recovery in men with localized prostate cancer receiving temporary ADT was assessed. Methods: A globally federated health research network (TriNetX) was used to identify men diagnosed with prostate cancer undergoing temporary ADT. Inclusion criteria consisted of: a clinically localized prostate cancer and eugonadal mean baseline T level (>300 ng/dL). Prior to starting ADT two cohorts were identified: Men receiving LHRH antagonists or LHRH agonists and men receiving combined ADT (LHRH agonist and antiandrogens). Further stratification was based on treatment duration of 6 months (short-term) or 18 months (long-term) to compare T recovery profiles 5 years after ADT cessation. Results: A total of 28,583 men received LHRH agonist or antagonist therapy alone and 20,188 men received combination ADT. A total of 46.7% of men who received short-term LHRH agonists or antagonists and 40.6% of men who received short-term combined ADT recovered to mean baseline T levels at 5 years (p = 0.06). Only men who received short-term LHRH agonist/antagonists recovered to a mean eugonadal level at 5 year follow-up. Meanwhile, 50% of men who received long-term LHRH agonist/antagonist therapy and 10.7% of men who received long-term combined ADT recovered to mean baseline T levels at 5 years (p < 0.0001). However, neither group recovered to a mean eugonadal T level. Conclusions: Most patients failed to recover to mean baseline and eugonadal T levels at 5-year follow-up. Given that TD is associated with a myriad of adverse effects such as metabolically adverse changes in body composition, increased insulin resistance, impaired bone health, and hypogonadal symptoms, serum T levels must be closely followed in men receiving ADT following treatment cessation. SOURCE OF Funding: NIH Grant R01 DK130991 and Clinician Scientist Development Grant from the ACS to RR