Session: MP80: Prostate Cancer: Localized: Surgical Therapy IV
MP80-14: Extraperitoneal Single-Port Robotic Radical Prostatectomy in Over 700 Patients: Updated Multi-Institutional Cohort Study from the SPARC Collaboration
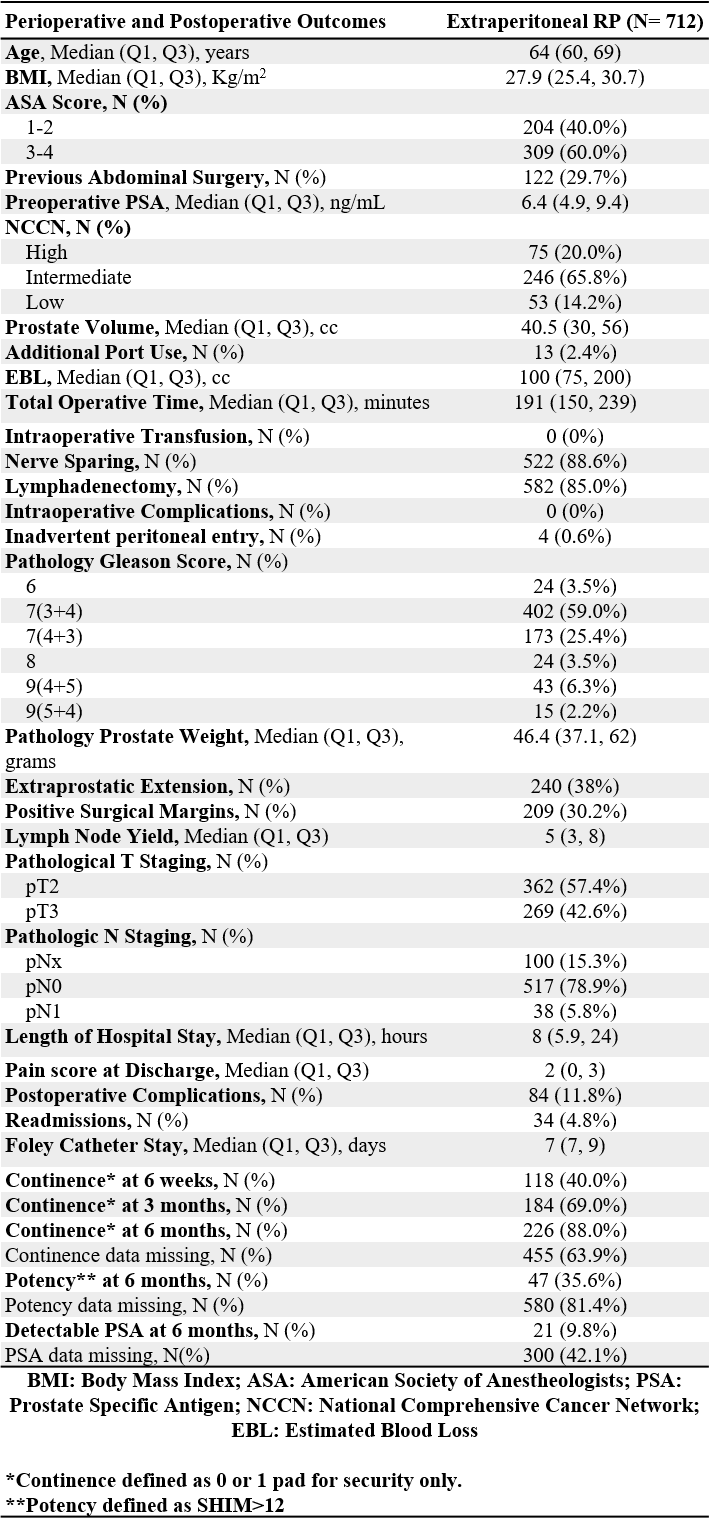
Introduction: An extraperitoneal approach to single-port (SP) robot-assisted radical prostatectomy has been demonstrated with proposed benefits in decreased morbidity, single incision, and same-day discharge. We sought to determine the perioperative and early postoperative outcomes in a large, multi-institutional setting. Methods: SP extraperitoneal radical prostatectomy was performed in 712 patients between February 2019 and October 2022. All procedures were performed by experienced robotic surgeons from eight tertiary medical centers. Data from baseline demographics, perioperative and early postoperative outcomes were collected prospectively and analyzed retrospectively Results: All reported procedures were completed without open conversion, blood transfusions, or intraoperative complications. The median follow-up time was 11.7 months for the entire cohort. The median age, BMI and preoperative PSA were 64 years, 27.9kg/m2, and 6.4 ng/mL, respectively. About 30% of the patients had at least one previous abdominal surgery. On pathology, high risk disease was noted in 12% and lymph node involvement on final pathology was present in 5.8%. Extraprostatic extension was noted in 38% and positive surgical margins were present in 30.2% of cases. Lymphadenectomy was performed in 85% of patients and the median lymph node yield was 5 nodes. There were no intraoperative complications and inadvertent peritoneal entry with insufflation was rare (0.6%) and managed conservatively. Postoperative complications occurred in 11.8%. The median length of stay and foley catheter duration were 8 hours and 7 days, respectively. Postoperative recovery of continence was 69% at 3 months and 88% at 6 months. Recovery of potency was 35.6% at 6 months. Conclusions: Single-port extraperitoneal robotic radical prostatectomy is safe and feasible for management of clinically localized prostate cancer. Analysis from a large multi-institutional cohort shows promising single incision and short hospital length of stay without compromise in early functional or oncologic outcomes. SOURCE OF Funding: None

 photo")