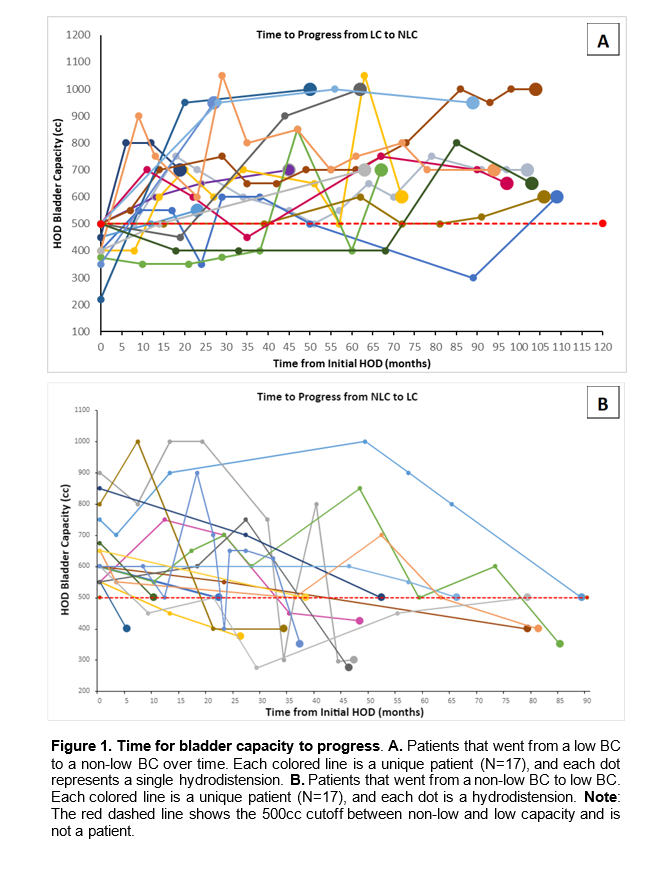
Introduction: Although therapeutic hydrodistension (HOD) is a level 3 treatment recommendation for patients with interstitial cystitis/bladder pain syndrome (IC/BPS), administration of the procedure varies among practitioners and the degree of therapeutic benefit is still an open question. The objective of this study was to use repeat bladder HOD data from a single clinical site to investigate longitudinal changes in anesthetic bladder capacity (BC) as a proxy for either improvement and/or bladder-centric disease progression. Methods: IC/BPS patients who underwent therapeutic HOD at our institution between 2009-2022 were identified through chart review. Only patients with 2 or more HOD were included in the analysis. All BCs were measured following HOD (100 mL H20 for 5 minutes). Results: A total of 1066 HOD in 221 unique patients was reported within the study window. Mean BC for all patients at first HOD was 795.5 cc (±320.11) and 813.7 cc (±356.41) at last HOD, with an average ?BC of 40.93 cc (p=0.573). In 95/221 (43%) patients, BC increased from first to last HOD. In 126/221 patients (57%), BC either stayed the same or decreased from first to final HOD. The difference in ?BC between these 2 groups was significant (p < 0.001). For 17/49 patients initially in the low-BC (defined here as BC = 500 cc) group, BC increased over time such that they were no longer considered low-BC at their last HOD (Figure 1A), whereas 17 patients with a non-low BC (i.e., >500 cc) at first HOD had joined the low-BC subgroup at the time of their final HOD (Figure 1B). Conclusions: The average change in BC across a large cohort of IC/BPS patients that underwent multiple HOD was minimal, however within this cohort there were two small but distinct subgroups: one for which BC increased over time from the low BC range into the non-low BC range, suggesting there may be some improvement in bladder properties, and a second group for which BC decreased over time and stayed in the low BC (i.e., bladder-centric) range, which may be indicative of disease progression. SOURCE OF Funding: R01 DK124599