Michigan State University College of Human Medicine
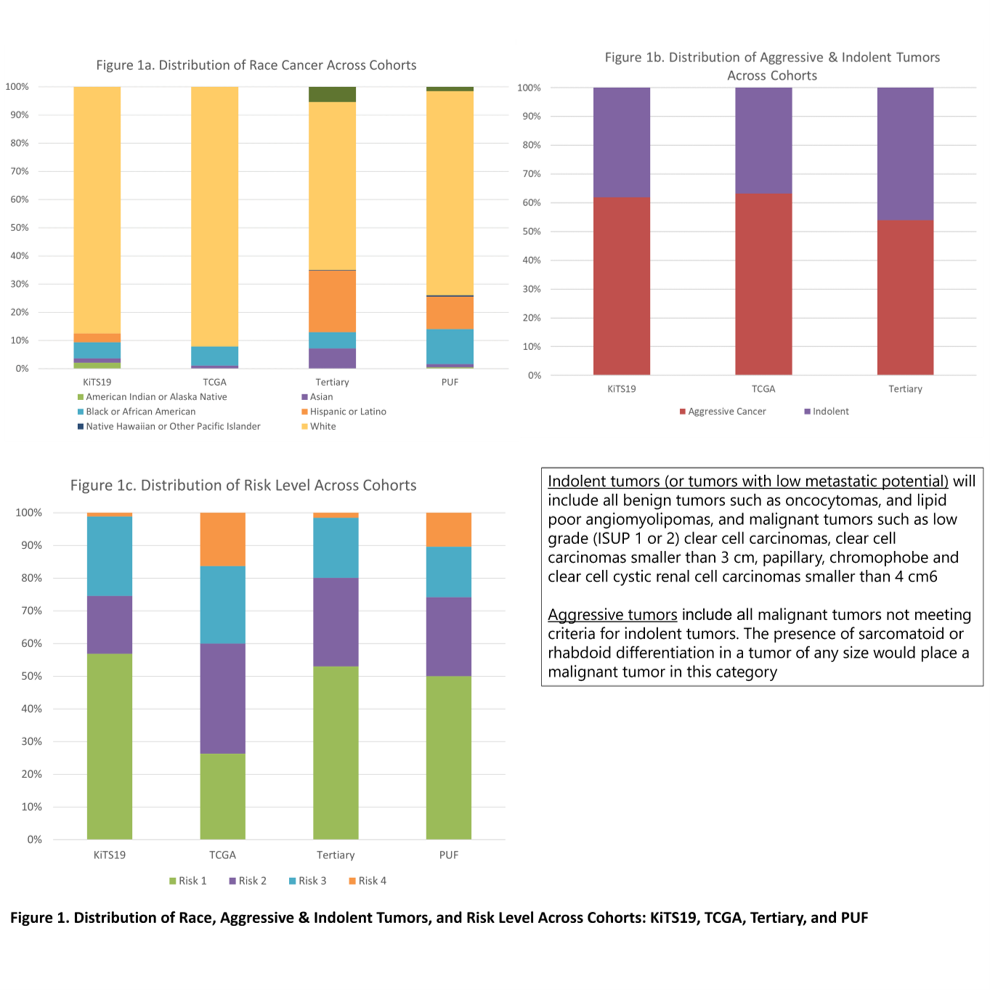
Introduction: We examine the heterogeneity and distribution of the cohort populations in two publicly used radiological image cohorts (Cancer Genome Atlas Kidney Renal Clear Cell Carcinoma (TCIA TCGA KIRC) collection and 2019 MICCAI Kidney Tumor Segmentation Challenge (KiTS19) used by AI researchers, and deviations in real world renal cancer data from population data from National Cancer Database (NCDB) Participant User Data File (PUF) and tertiary cancer center data. PUF data is used as an anchor for prevalence rate bias assessment. Specific gene expression and therefore biology of RCC differ by race especially between the Black and White population. AI algorithms learn from datasets, but if the dataset misrepresents the population, reinforcing bias may occur. Ignoring these demographic features will incur inaccurate prognostication, thereby limiting the translation of these analyses to clinical practice. Consciousness of model training biases is vital to patient care decisions when using models in clinical setting. Methods: Data evaluated included the gender, demographic and reported pathologic grading and staging. American Urological Association (AUA) risk levels were used. Poisson regression was used to estimate the population-based and sample specific estimation for prevalence rate and corresponding 95% confidence interval. SAS 9.4 was used for data analysis. Results: Compared to PUF, KiTS19 and TCGA KIRC over sampled White by 9.5% (95% CI, -3.7% to 22.7%) and 15.1% (95% CI, 1.5% to 28.8%), under sampled Black by -6.7% (95% CI, -10% to -3.3%), -5.5% (95% CI, -9.3% to -1.8%). Tertiary also under sampled Black by -6.6% (95% CI, -8.7% to -4.6%). The tertiary cohort largely under sampled aggressive cancers by -14.7% (95% CI, -20.9% to -8.4%). No statistically significant difference was found among PUF, TCGA, and KiTS19 in aggressive rate, however heterogeneities in risk are notable. TCGA and KiTS19 largely oversampled high-risk tumors with the oversampling rate of 3% (95% CI, 1.3% to 15.2%), 5.9% (95% CI, 0.2% to 11.7%) for TCGA and 8.3% (95% CI, 1.3% to 15.2%), 5.9% (95% CI, 0.2% to 11.7%) for KiTS, in risk level 3 and 4, respectively. Conclusions: Heterogeneities between surgical and oncological cohorts need to be considered in future AI training and cross-validation for renal masses. SOURCE OF Funding: N/A