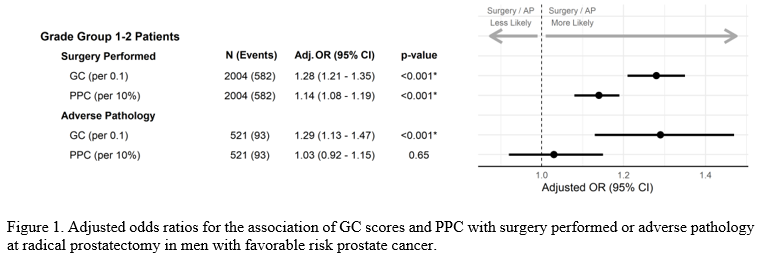
Introduction: The Surveillance, Epidemiology, and End Results (SEER) cancer registry was linked to the Decipher 22-gene expression classifier (GC) for men with prostate cancer (PCa). We examined the use of conservative management (active surveillance/watchful waiting) for GC tested and untested men and assessed factors associated with adverse pathology (AP; grade group =3, pathological stage =pT3b, or lymph node invasion) at radical prostatectomy (RP). Methods: Men in the registry diagnosed with favorable risk (grade group [GG] 1 and 2) PCa from 2016 to 2018 were linked to data from GC testing conducted between 2016 to 2020 (Veracyte, San Diego, CA). GC scores (range 0-1) and GC risk groups (low, intermediate, and high) were used for continuous and categorical analyses. Multivariable logistic regressions quantified the association of GC test results with conservative management as well as the association of GC test results with AP at RP in comparison to tumor volume as measured by the percentage of positive cores with cancer (PPC). Results: A total of 100,279 men were evaluated (2,889 tested with GC at biopsy and 97,390 untested). Overall, conservative management increased from 20% to 23% and 33% to 37% from 2016 to 2018 in the untested and tested populations, respectively. In men aged <70 years, conservative management increased from 20% to 24% and 35% to 37% from 2016 to 2018 in the untested and tested populations, respectively. In adjusted analyses, GC testing was significantly associated with greater odds of conservative management (OR [95% CI] 2.1 [1.9-2.4], p<0.001). Conservative management use was highest for GC low risk men (41%) as compared to intermediate (31%) or high (16%) GC risk men. Higher GC and PPC were associated with RP surgery; but for men treated with RP, only higher GC was significantly associated with adverse pathology (Figure 1). Conclusions: GC testing was independently associated with a two-fold increase in conservative management utilization for favorable risk disease. Men with lower GC scores were more likely to undergo conservative management. Both higher GC scores and tumor volume (as measured by PPC) were associated with increased likelihood of RP. Higher GC was significantly associated with a higher likelihood of AP at time of RP, while higher tumor volume was not. SOURCE OF Funding: There was no direct funding from an outside organization or sponsor.

.jpg "Alec Zhu, MD (he/him/his) photo")