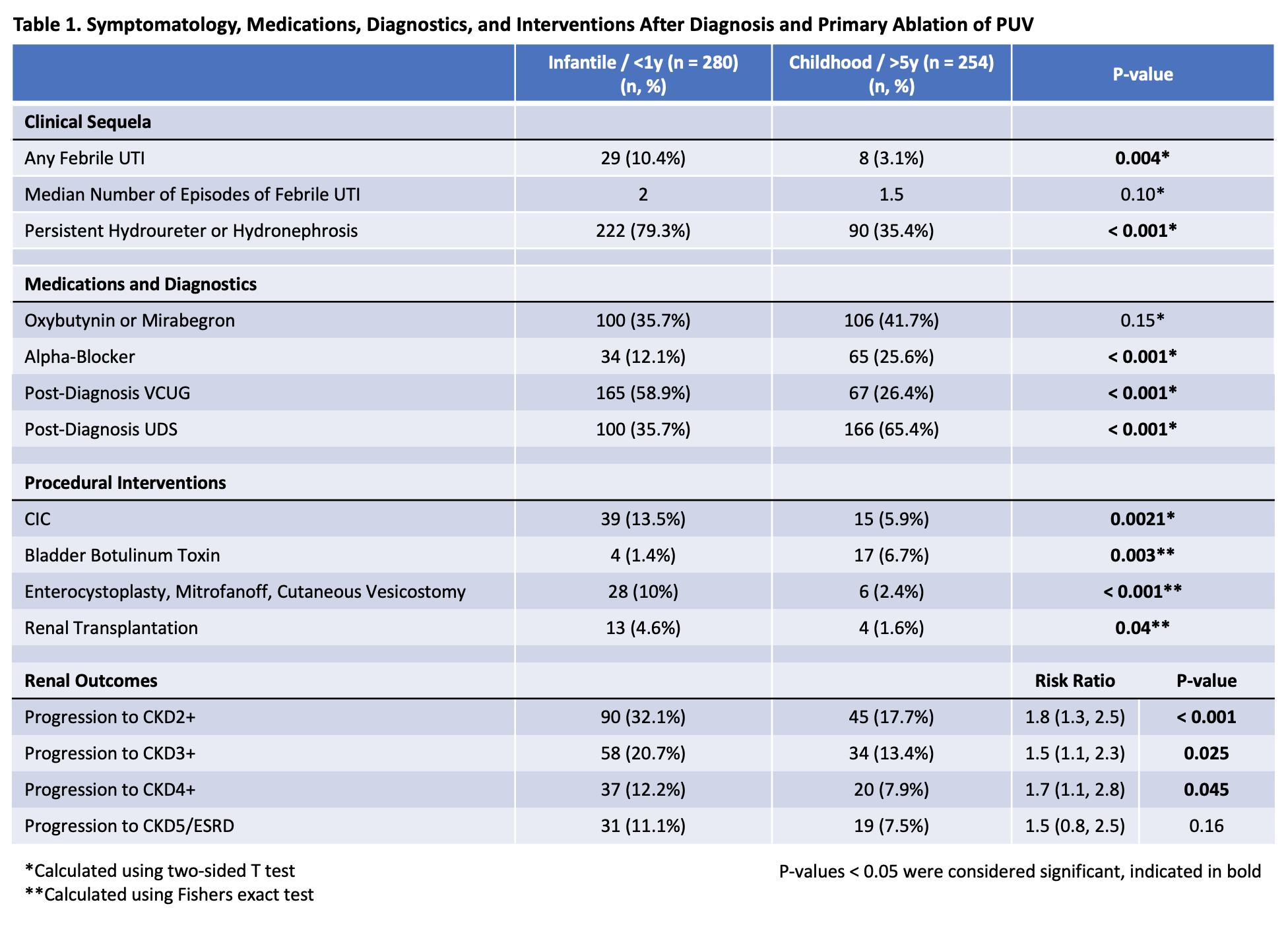
Introduction: Management patterns and clinical outcomes are poorly defined in cases of late PUV diagnosis. Studies have debated whether a late diagnosis portends a favorable outcome due to milder obstructive uropathy or a worse outcome due to prolonged obstruction. We compare post-ablation management and clinical outcomes of infantile ( <1y) versus childhood (>5y) PUV diagnosis to gain insight into the pathologies at opposite ends of the PUV spectrum. Methods: A retrospective cohort study was conducted using the TriNetX research network between 2006-2022. We defined two cohorts: 1) The <1y arm had an index diagnosis of PUV (Q64.2) and cystoscopy with valve ablation (52400) within 1 year of life, 2) the >5y arm had an index diagnosis of PUV and valve ablation after age 5. We report rates and time-to-first use of anticholinergic/B3 agonists, alpha-blockers, clean intermittent catheterization (CIC), bladder botox, enterocystoplasty/Mitrofanoff, as well as progression of CKD. Results: We identified 534 patients (280 <1y; 254 >5y). Median age at diagnosis was 1 month and 9 years for the <1y and >5y cohorts, respectively. Median follow-up was 8 and 10 years for the <1y and >5y cohorts. The <1y arm was significantly more likely to have persistent hydronephrosis (79.3% vs 35.4%) as well as any febrile UTI (10.4% vs 3.1%) (Table 1). Following ablation, patients in both arms were primarily managed with anticholinergic/B3 agonists, with no difference between groups (35.7% vs 41.7%). The >5y arm was significantly more likely to receive alpha-blockers (25.6% vs 12.1%) or bladder botox (6.7% vs 1.4%). The <1y arm was significantly more likely to be started on CIC, undergo enterocystoplasty or Mitrofanoff, or renal transplant. The <1y arm had significantly higher rates and shorter time-to-progression to CKD2+, CKD3+, and CKD4+. There were similar rates of ESRD (Table 1). Conclusions: Patients with a late PUV diagnosis are disproportionately managed with conservative strategies (antispasmodics, bladder botox). Despite higher utilization of conservative strategies, the late diagnosis cohort had superior renal outcomes and low rates of progression to invasive treatments. The findings present compelling evidence that, with few exceptions, a late diagnosis reflects an overall milder disease process. SOURCE OF Funding: NA

 photo")