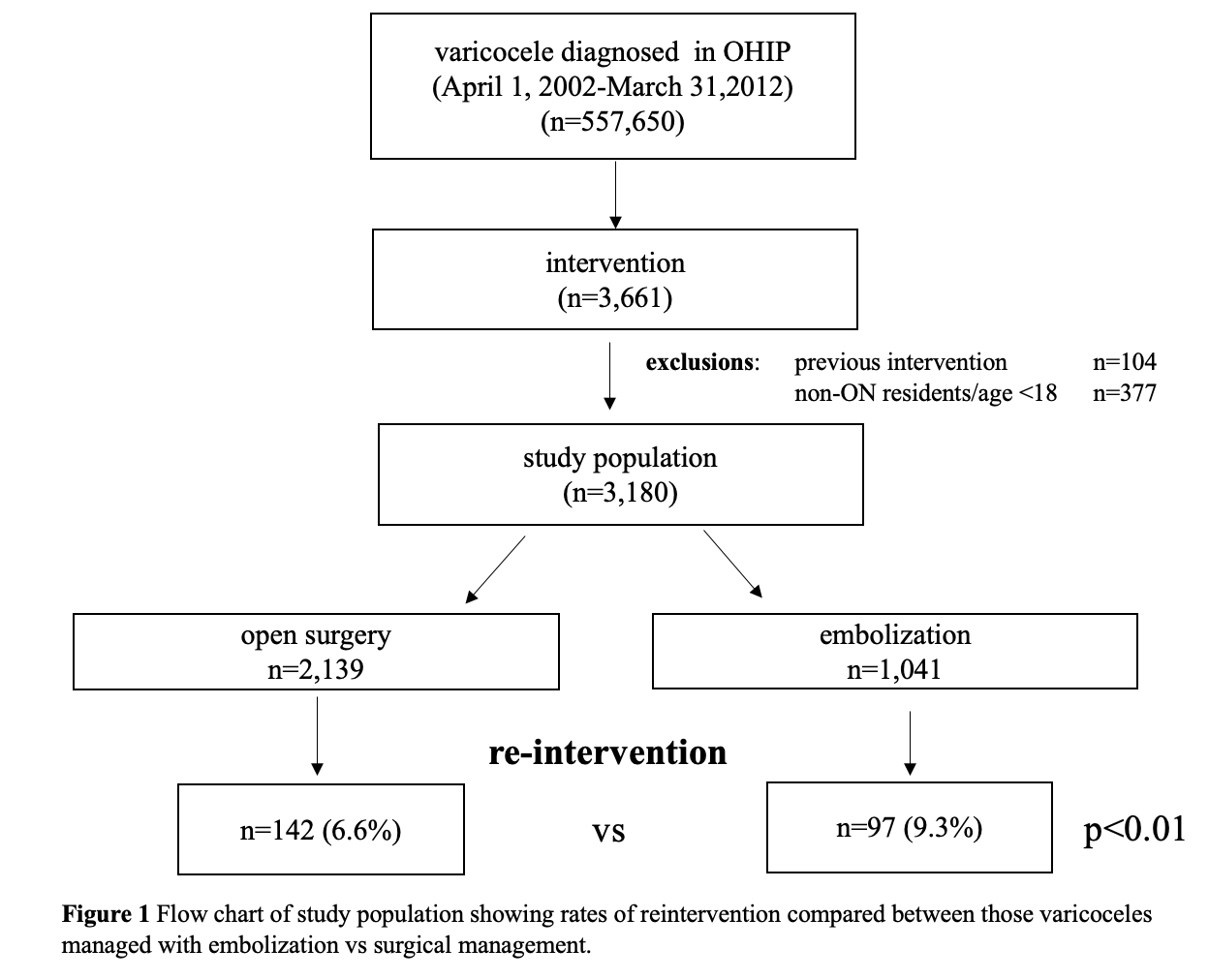
Introduction: The optimal approach for management of varicocele is currently unknown. Existing evidence is of low quality with no randomized controlled studies comparing approaches. We provide the first population-based analysis of embolization vs surgical management of varicocele. Methods: All patients in the province of Ontario who underwent treatment of their varicocele between April 1, 2002-March 31, 2012 were identified using ICES databases. The index intervention was considered the approach first used in the treatment-naïve patient – open surgery or embolization. The primary outcome was the rate of reintervention while secondary outcomes included complications and healthcare utilization. Results: We identified 557,650 male patients with a varicocele diagnosis, of whom n=3,180 underwent an intervention and were included in the study – n=2,139(67%) underwent open varicocelectomy while n=1,041(33%) underwent embolization as their index intervention (Figure 1). Reintervention was more common amongst those who underwent embolization compared to those who underwent surgical management [n=97(9.3%) vs n=142(6.6%);p < 0.01]. While controlling for demographics, regression analysis showed surgical varicocelectomy was still less likely to require reintervention [OR 0.68(0.52-0.90);p < 0.01]. Those who underwent surgical management had higher rates of complications requiring ED visits within 1 month of the procedure. This association was persistent on regression analysis, controlling for demographics [OR 1.69(1.27-2.25);p < 0.01]. There was no difference in hospital admissions between the groups [OR 1.53(0.94-2.49);p=0.087]. There was a weak association between socioeconomic status (SES) and type of index intervention with the least wealthy income quintile more likely to receive surgery [OR 1.27(1.01-1.60);p=0.04] while there was no difference based on rurality and age. Conclusions: This first population-based study to examine surgical management vs embolization for treatment of varicocele shows that surgery is less likely to require repeat intervention but with a modest increased risk of complications. SOURCE OF Funding: NA