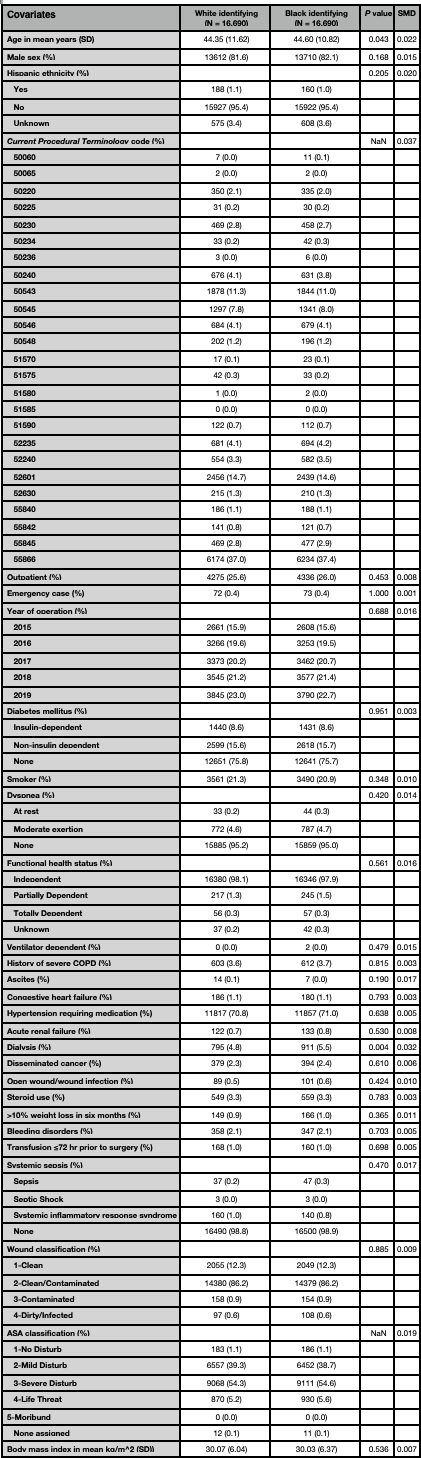
Introduction: Diversity, equity, and inclusion is a priority in healthcare. Despite this mission, there is limited literature on race and post-operative complications in urology. Methods: Adult patients undergoing urologic surgeries (i.e., nephroureterectomy, radical prostatectomy, radical cystectomy, radical and partial nephrectomy, and percutaneous nephrolithotomy) between 2015 to 2019 were identified from NSQIP. Black-identifying patients were matched with White-identifying patients using a 1:1 nearest-neighbour propensity-score matching protocol including surgical procedure and baseline variables that were significantly different between groups. Between group comparisons were estimated using logistic regression and presented as odds ratios (OR) with 95% confidence intervals (CI) and p-values. Results: A total of 138,777 individuals that underwent urologic procedures were identified (48.3±11.5 years, 83.2% male, 12.1% Black-identifying). After matching, a well-balanced cohort of 33,380 patients were included for analysis (Table 1). Medically, Black-identifying patients were more likely to be diagnosed with pneumonia (OR: 1.31, 95% CI[1.03–1.66], p=0.029), have unplanned reintubation (OR: 1.48, 95% CI[1.12–1.97], p=0.006), have a ventilator for >48 hours (OR: 1.49, 95% CI[1.05–2.14], p=0.027), have progressive renal insufficiency (OR: 1.72, 95% CI[1.32–2.26], p<0.001), acute renal failure (OR: 1.49, 95% CI[1.07–2.07], p=0.018), and bleed requiring transfusion (OR: 1.11, 95% CI[1.01–1.21], p=0.035) compared to White-identifying patients. Black-identifying patients were less likely to be diagnosed with myocardial infarction (OR: 0.63, 95% CI[0.42–0.94], p=0.024). Surgically, Black-identifying patients were less likely to be diagnosed with a superficial surgical site infection (SSI) (OR: 0.68, 95% CI[0.52–0.88], p=0.003). Conclusions: Black-identifying patients undergoing urologic surgery were significantly more likely to have respiratory, renal, and bleeding complications and less likely to be diagnosed with myocardial infarction and superficial SSI. Although this raises questions about health equity in urology, more research is needed. Confounders such as socioeconomic status and access to care were not measured. SOURCE OF Funding: None.

 photo")