Session: MP11: Prostate Cancer: Advanced (including Drug Therapy) I
MP11-08: Exploring the Effect of Metastasis Directed Therapy on Progression Patterns of Patients with Positive 68Ga-PSMA PET/CT and Biochemical Recurrence from Prostate Cancer.
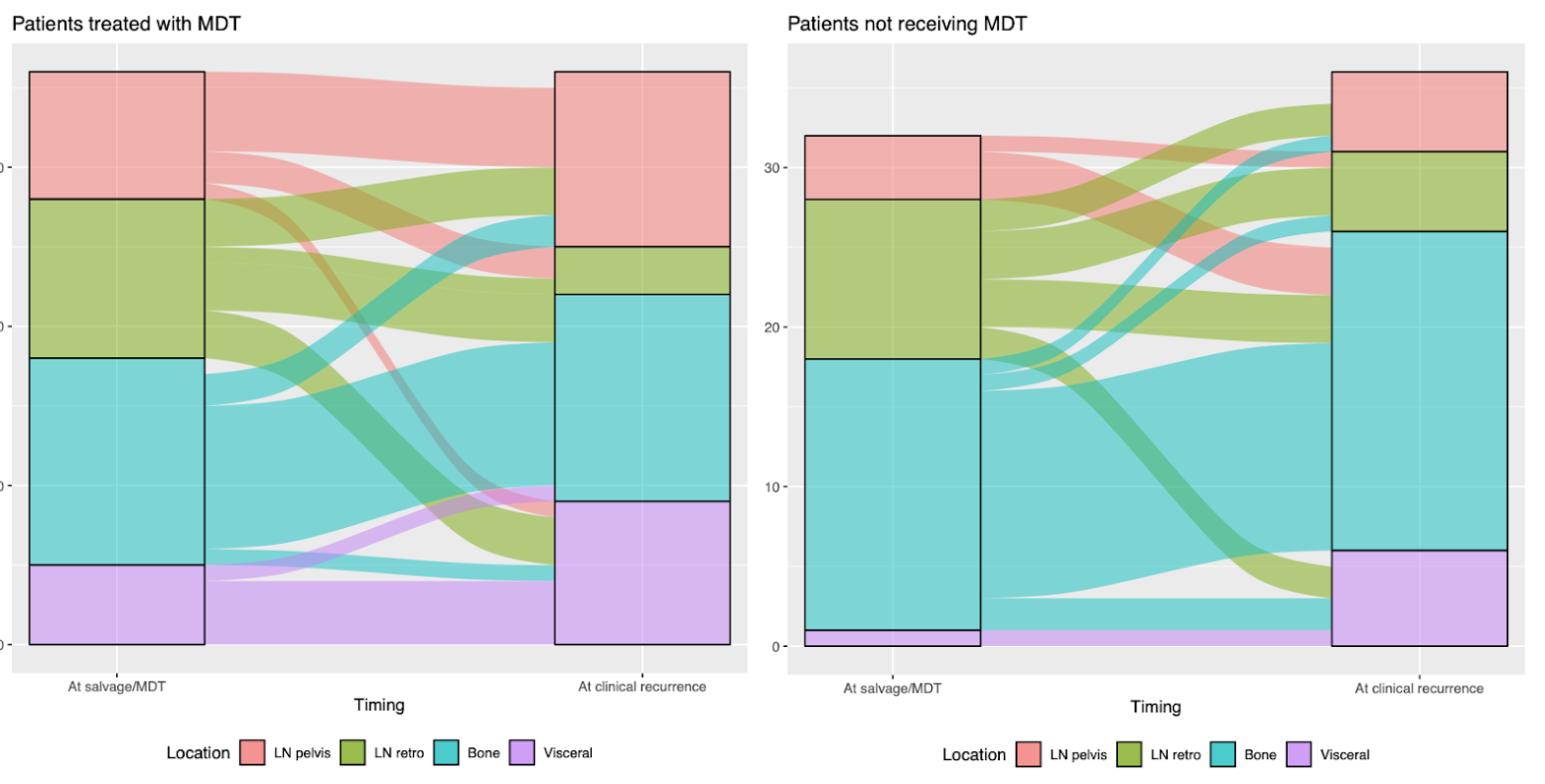
Introduction: In men with positive PSMA PET for biochemical recurrence (BCR) after radical prostatectomy (RP), metastasis directed therapy (MDT) may represent a treatment option. However, there is little evidence regarding the role of MDT in terms of prognostic implications as well as on the patterns of subsequent clinical recurrence (CR). Methods: We retrospectively identified 226 patients with positive 68Ga-PSMA PET at BCR after RP between 2016 and 2022 at a single Institution. MDT consisted of stereotactic ablative radiation therapy on positive spots, either nodal, bony or visceral. CR was defined as any new metastases detected at imaging after a first PSMA PET. Patients were stratified according to the use of MDT (n=109) vs. no MDT (n=117). Kaplan-Meier analyses assessed time to CR. Per-lesion analysis using Pearson Chi-square assessed the impact of MDT on the location of CR after a positive PSMA PET. The variation of the site of recurrence compared to the location of positive spots at first PSMA PET (pelvic vs non-pelvic distant spots) was tested and represented using alluvial plots. Results: At median follow-up of 24 months after the first PSMA PET, 73 patients had CR. The 3-year CR-free survival rates were 51 vs. 28% for MDT vs. no MDT. The distribution of positive spots location at first PSMA PET did not differ between men receiving or not MDT (pelvic 19% vs 22%, retroperitoneal 19% vs 15%, bone 38% vs 34%, visceral 13% vs 12%, p=0.6). Similarly, in men with CR after a positive PSMA PET (n=73), no statistically significant differences in terms of site of CR were observed based on MDT use (pelvic 29% vs 14%, retroperitoneal 8% vs 14%, bone 35% vs 55%, visceral 24% vs 17%, p=0.4). However, while a significant increase in rate of distant metastases at CR was reported in men not receiving MDT compared to the pre-MDT PSMA PET (from 77 to 86%), a reduction in proportion of distant metastases at CR was observed in patients receiving MDT (from 76 to 67%) (Fig 1) Conclusions: The use of MDT represents a protective factor for metastases during follow-up. Interestingly, the pattern of recurrence was influenced by the use of MDT with lower rate of CR to non-pelvic distant sites. Salvage therapies might alter patterns of PCa dissemination. SOURCE OF Funding: none