Session: MP11: Prostate Cancer: Advanced (including Drug Therapy) I
MP11-11: Tailoring the optimal use of Androgen-Deprivation Therapy concomitant to post-operative Radiotherapy among men with pN1 prostate cancer. Long-term results of a large, single Institution series.
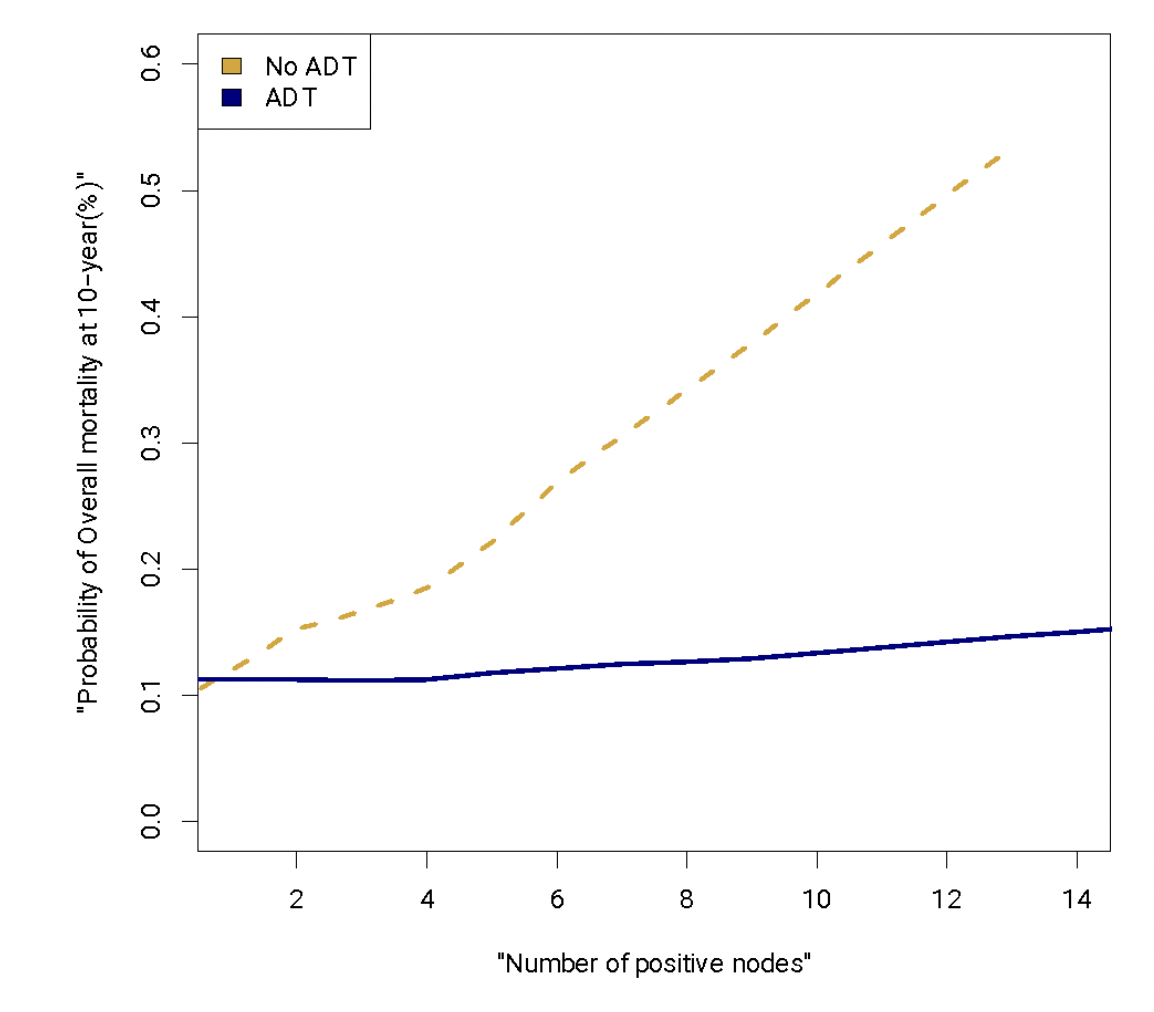
Introduction: The role of androgen-deprivation therapy (ADT) during adjuvant (aRT) or salvage radiotherapy (sRT) in men with node-positive prostate cancer is still debated. In particular, it is unclear whether adding ADT may provide further benefit based on the metastatic nodal burden. We aimed at exploring the correlation between ADT and the number of positive nodes at pathology and its impact on survival. Methods: 8,362 patients treated with RP at a single center between 1987 and 2020 were identified. Only patients with lymph node invasion (LNI) treated with aRT or sRT for BCR were included, resulting in 710 eligible men. The endpoint was overall mortality (OM). The probability of receiving ADT was weighted through an inverse-probability of treatment and the resulting weight was used as propensity adjustment in Cox regression models testing the impact of ADT on OM after further adjustment for age, RT type, adverse pathology and number of positive nodes. An interaction term tested the correlation between ADT and number of positive nodes on OM and the result was represented using Lowess. Results: Of 710 patients, 578 (81%) vs 132 (19%) men received aRT vs sRT, respectively, and 559 (78%) received ADT. Median follow-up was 116 months. A total of 112 patients died during follow-up. The 10-year overall survival rate was 82%. At Cox analyses, ADT use was associated with reduced risk of OM (HR 0.61, p = 0.042). Similarly, higher metastatic nodal burden was associated with increased risk of OM (HR 1.02, p=0.001). The interaction terms confirmed a significant interaction between ADT use and number of positive nodes (p=0.02). At Lowess, ADT did not provide a survival benefit in patients with a single positive node (10 vs. 12% 10-yr OM in no ADT vs ADT group). Conversely, not administering ADT with increasing metastatic nodal burden was associated with higher risk of OM (from 14 to 28% 10-yr OM in patients with 2 to 6 positive nodes), while OM rates remained stable at 12% when ADT was administered. Conclusions: Among patients with LNI undergoing salvage or adjuvant RT, the use of concomitant ADT can be omitted in case of a single metastatic node. Conversely, ADT use provides a significant survival benefit in patients with higher metastatic nodal burden. SOURCE OF Funding: none

 photo")