Session: MP67: Prostate Cancer: Localized: Surgical Therapy III
MP67-04: Validation of Novel Preoperative Risk Categories On The Prediction of Clinical Recurrence In Patients Candidate for Radical Prostatectomy For clinically localized Prostate Cancer. Results of a large, multi-institutional series.
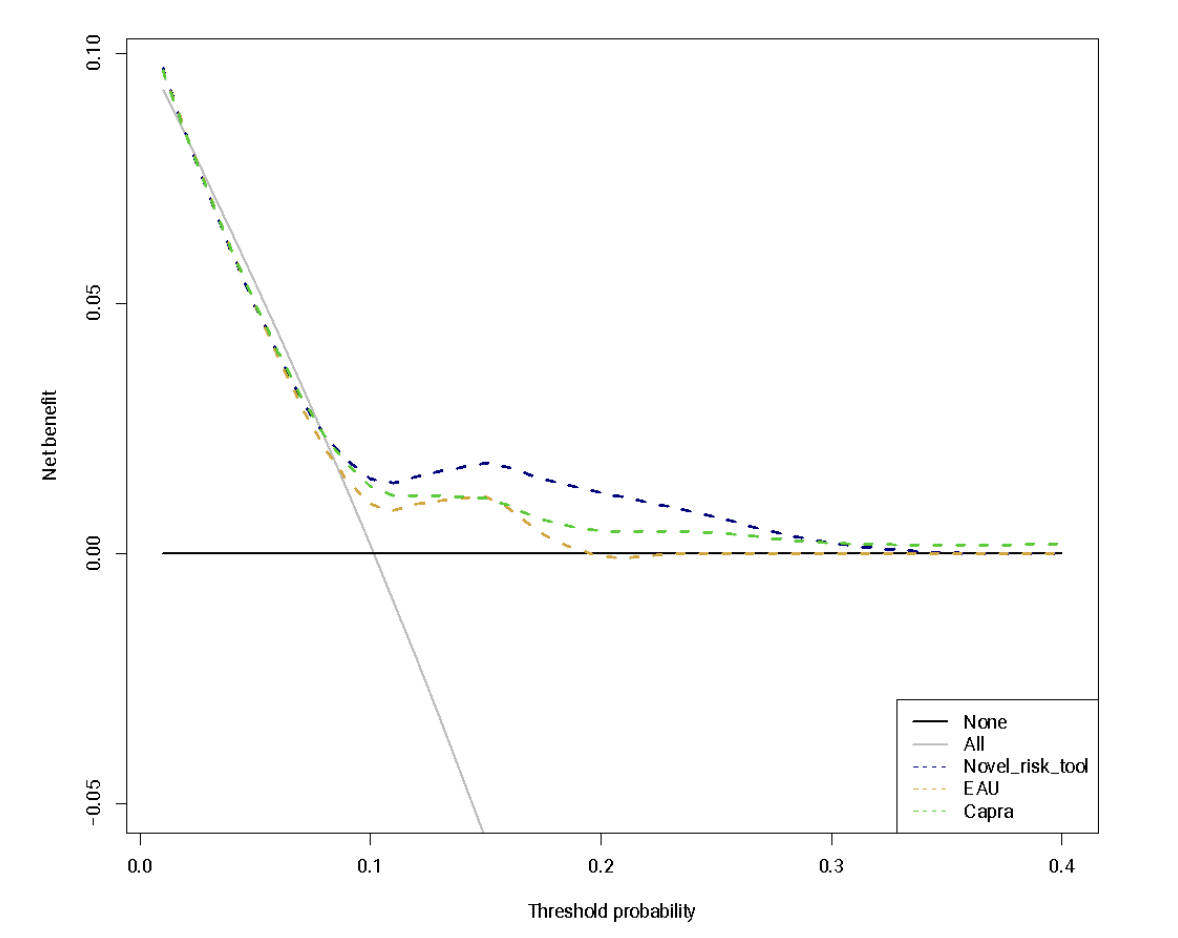
Introduction: Most of the preoperative risk tools predicting prostate cancer (PCa) recurrence after radical prostatectomy (RP) considered biochemical recurrence (BCR) as the main endpoint when developed. However, not all patients with a BCR ultimately progress to clinical recurrence (CR). We aimed at internally validating a novel preoperative risk classification in predicting CR in patients treated with RP. Methods: Overall, 2,901 patients treated with RP and who received pre-op mpMRI between 2014 -2022 at eight referral centers were identified. The study outcome was 5-yr CR defined as positive imaging after BCR. Kaplan-Meier and multivariable Cox regression models tested time and predictors of CR. Predictors consisted of PSA, biopsy grade group, MRI stage (organ-confined vs extracapsular extension vs. seminal vesicles invasion) and maximum diameter of lesion at MRI. These variables defined four risk groups based on the novel classification. The tool accuracy was compared to the EAU risk classification and CAPRA score in predicting 5-year CR using Harrel’s c-index. Decision curve analyses (DCA) compared the net-benefit associated with each of the risk tools. Results: Overall, 937 (32%), 1006 (35%), 848 (30%) and 110 (3%) had low, intermediate, high and very-high risk disease according to the novel classification. Median follow-up was 43 months. At KM analyses, 5-year CR-free survival rates were 94, 90, 83 and 71% in, respectively, low, intermediate, high and very-high risk groups (p < 0.01). The novel model tested for prediction CR in Cox regression analyses depicted good discrimination at internal validation (c-index 76%). After testing the accuracy of the EAU risk groups and the CAPRA score in our cohort, the novel model showed higher c index (78 vs. 69 vs. 73%). At DCA, our novel model showed a higher net-benefit compared to other models (Fig1). Conclusions: We internally validated a novel preoperative risk tool to predict CR after RP. Our model exhibited higher accuracy as compared to available tools in the prediction of stronger oncologic endpoints at mid-term follow-up. This data reinforces the utility of this patient stratification for preoperative counselling and outcome predictions. SOURCE OF Funding: no