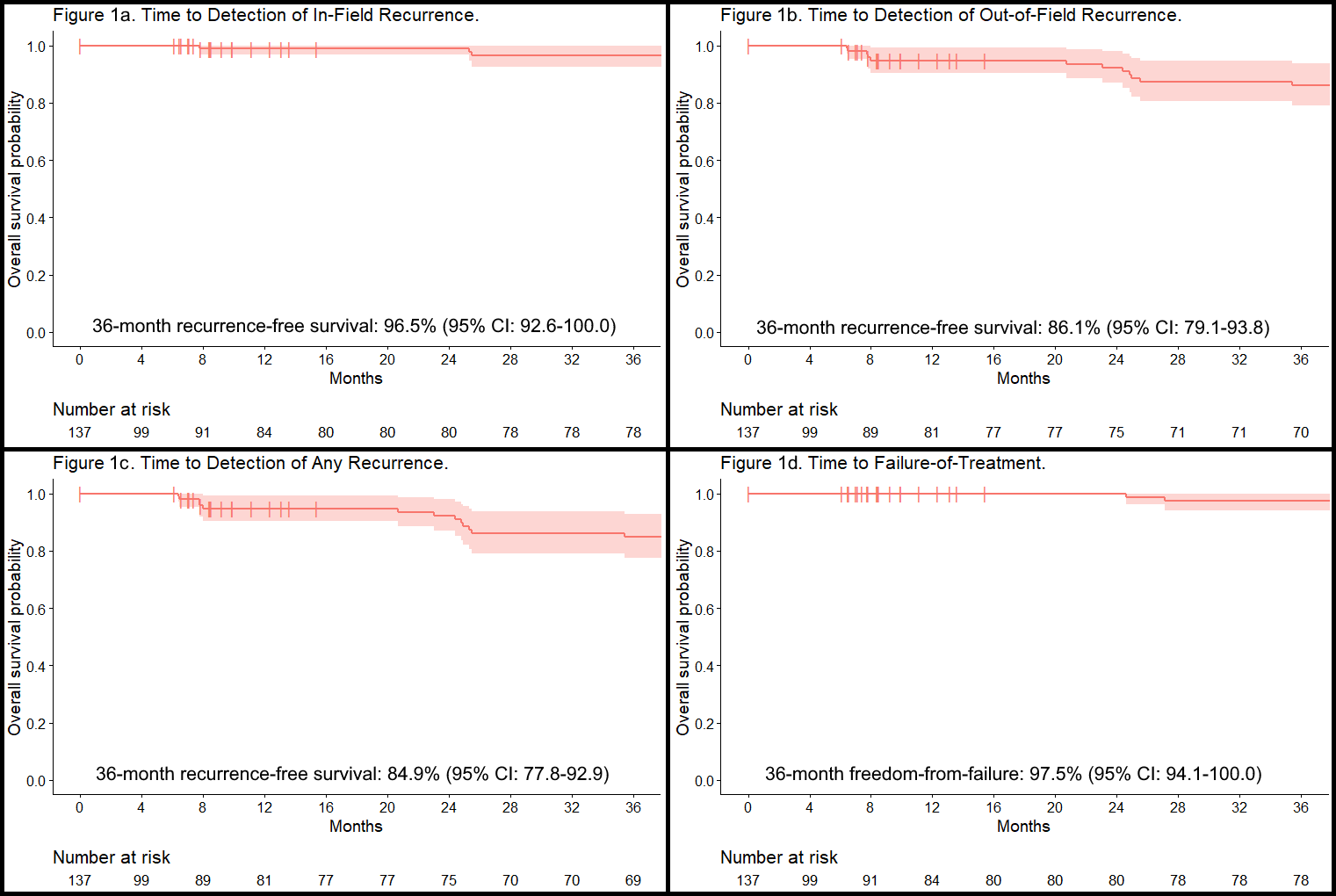
Introduction: mpMRI coupled with MR targeted biopsy reliably identifies candidates for PPGCA harboring unifocal clinically significant prostate cancer (csPCa). The present study reports 3-year oncological outcomes following PPGCA in a cohort of men with unilateral intermediate risk prostate cancer undergoing surveillance biopsies at 6 months and 2-years Methods: Men with unilateral intermediate risk prostate cancer undergoing PPGCA between 3/2017 and 5/2020 were enrolled in a prospective outcome registry. The post-ablation surveillance protocol for all men included PSA testing every six months and mpMRI at six months and 2 years. Surveillance prostate biopsy was initially recommended at six months and subsequently in all men at 2-years. Recurrence of csPCa was defined as any Gleason Grade Group >1 disease at any time point. Freedom-from-failure represented no whole-gland salvage treatment, metastatic prostate cancer, or prostate cancer mortality. Kaplan-Meier survival curves captured recurrence of csPCa and freedom-from-failure (Figure 1). Results: 122 men had at least 24 months of follow-up data. Surveillance biopsies identified csPCa in 13 (17.3%) of evaluable men. At 36 months, biopsy detection survival rate for in-field, out-of-field and overall csPCa was 96.1% (95% CI: 91.9-100.0), 84.8% (95% CI: 77.3-93.2), and 83.5% (95% CI: 75.6-92.2), respectively (Figure 1). The probability of freedom-from-failure at 36 months was 97.3% (95% CI: 93.6-100.0) (Figure 1). Of the 13 men with csPCa, 4,5,2 and 2 were managed with active surveillance, salvage PGCA, salvage RP and two refused whole gland treatment, respectively. The sensitivity of mpMRI for any csPCa was 38% Conclusions: The low in-field cancer detection rate at 3 -years indicates successful ablation of localized cancers. Conversely, the out-of-field detection rate of 15% highlights the need for continued surveillance The increasing time-dependent risk for detecting out of field csPCa emphasizes the need for long-term surveillance and identification of predictors of csPCa recurrences which would guide necessity and timing of surveillance biopsies. SOURCE OF Funding: None