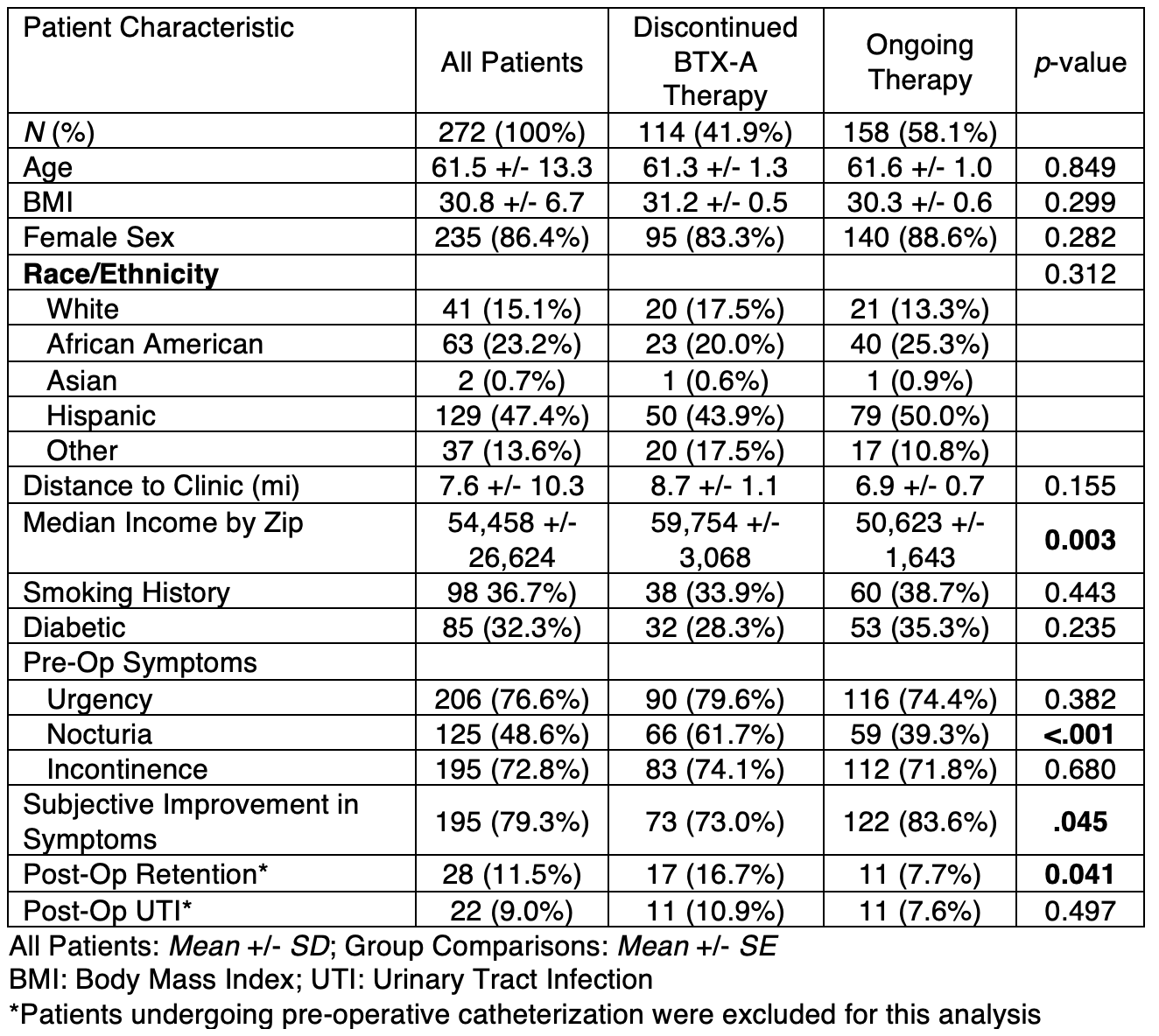
Introduction: Although overactive bladder (OAB) is a common condition affecting 16% of Americans, few patients continue second-line and third-line treatment. This study sought to investigate factors associated with discontinuation of intravesical Onabotulinom Toxin-A (BTX-A) injections among a diverse urban population. Methods: This was a retrospective review of patients who underwent BTX-A injection for OAB at a university hospital between November 2015 and December 2021. Patients were considered to have discontinued BTX-A therapy if they only received one treatment and it had been more than 1 year since last date of service. Patients with neurogenic OAB were excluded. Patient demographics, past medical history, symptoms, and post-operative outcomes were compared between groups with Chi-squared, Student’s t-test, or Fisher’s exact test. Results: BTX-A injections were administered to 272 patients who met study criteria of which 114 (41.9%) had discontinued BTX-A therapy. Our cohort included 235 (86%) women and had a mean age of 61.5 and mean BMI of 30.8. Patients discontinuing BTX-A therapy had a higher median income ($59K vs. $50K, p<.01) and were more likely to have reported nocturia (61.7% vs. 39.3%, p<.001). Patients who discontinued were less likely to have reported subjective improvement of symptoms at their first post-procedure visit (73.0% vs. 83.6%, p<.05). Similarly, patients who developed post-operative urinary retention were more likely to discontinue BTX-A therapy (17% retention in discontinuation group vs. 8% in those who continued p<.05). There were no associations between discontinuation and Race/Ethnicity, distance to clinic, smoking history, or post-operative urinary tract infections. Conclusions: Adverse outcome after BTX-A injection, such as post-operative urinary retention, is associated with discontinuation of therapy, whereas subjective improvement in symptoms is associated with continuation of therapy. Given the large proportion (>40%) of patients who discontinued BTX-A treatment, further research is needed to identify barriers to continuation of care. SOURCE OF Funding: None.