PD09-11: The immune-related adverse events paradox in locally advanced or metastatic urothelial cancer patients receiving atezolizumab: Analysis of individual participant data from IMvigor210 and IMvigor211
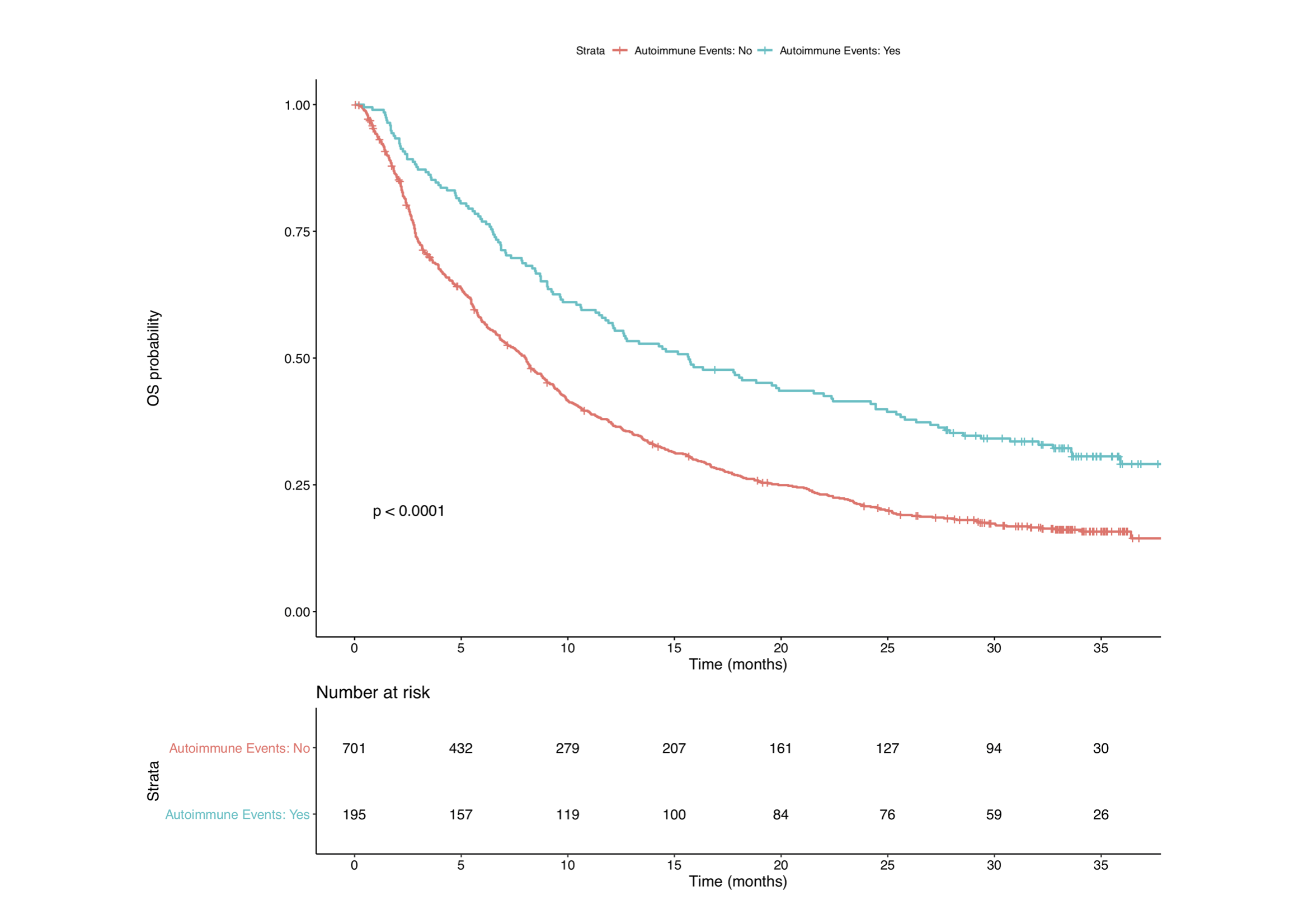
Introduction: Immune checkpoint inhibitors (ICIs) have changed the treatment landscape for advanced urothelial cancer; however, many patients are lost early during treatment follow-up and predictors of response at the patient and tumor level remain poorly understood. We investigated the association between immune-related adverse events (irAEs) and oncological outcomes in patients receiving ICIs, and whether the administration of systemic corticosteroids diminishes their impact. Methods: We relied on individual participant data from two prospective trials for advanced urothelial cancer: IMvigor210 and IMvigor211. A total of 896 patients who received Atezolizumab for locally advanced or metastatic urothelial carcinoma were considered. Data were used according to Hoffmann–La Roche policy and made available through Vivli, Inc. The association between irAEs occurrence and clinical progression-free survival (PFS), overall survival (OS), and cancer-specific survival (CSS) was tested by means of multivariable Cox or competing-risks regression, when appropriate. Moreover, patients experiencing irAEs were further stratified based on systemic corticosteroids administration. Results: On multivariable analysis, irAEs were inversely associated with the risk of disease progression [HR 0.50 95% CI (0.40-0.61) p<0.001], overall mortality [HR 0.51 95% CI (0.41-0.64) p<0.001], and cancer-specific mortality [SHR 0.55 95% CI (0.45-0.72) p<0.001]. Moreover, the administration of systemic corticosteroids was not associated with worse oncological outcomes [PFS: HR 0.92 95%CI (0.62-1.34), p= 0.629; OS: HR 0.86 95% CI (0.51-1.64), p= 0.613; CSS: SHR 0.90 95% CI (0.60-1.36), p=0.630]. Conclusions: The development of related irAEs while receiving atezolizumab treatment was associated with improved oncological outcomes. These findings seem to not be affected by systemic corticosteroids administration. SOURCE OF Funding: none