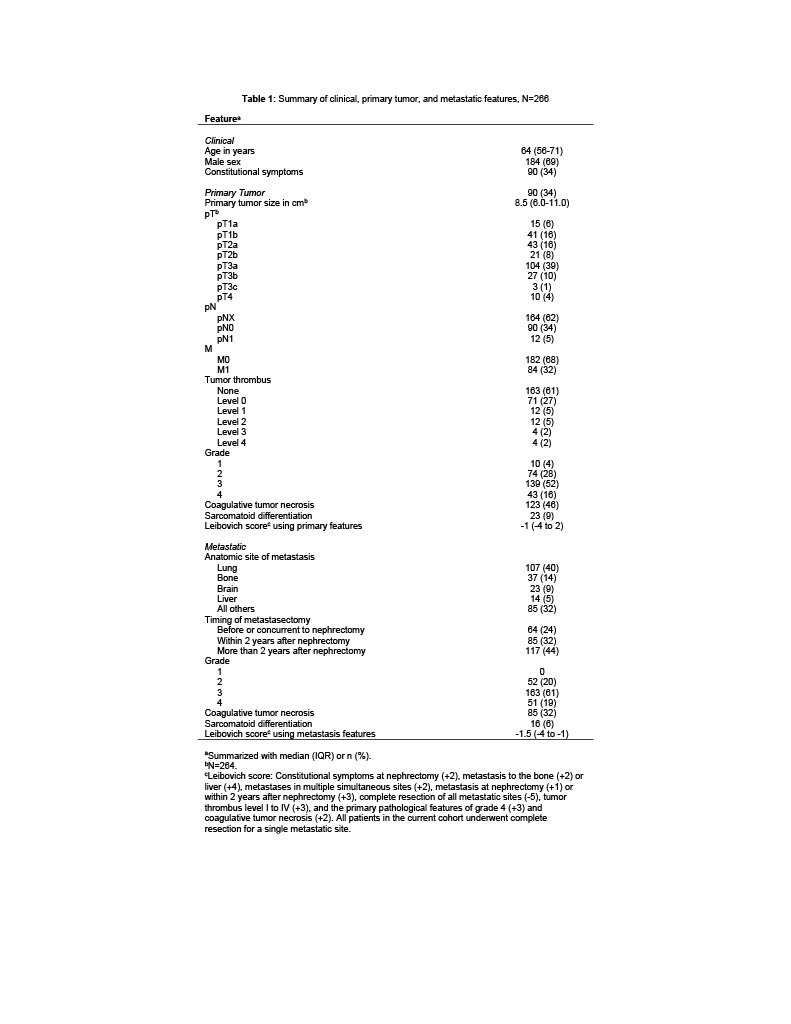
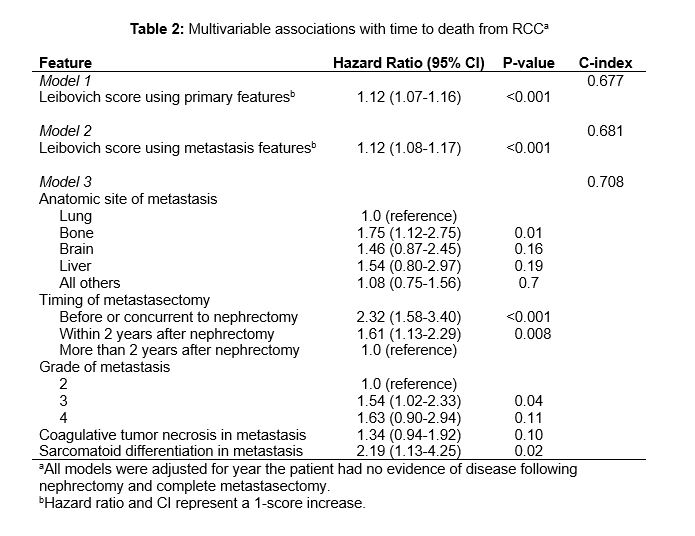
Introduction: Multiple prognostic models exist to assess survival among patients with metastatic clear cell renal cell carcinoma (m-ccRCC). However, the relative contribution of metastasis histopathology to model performance has not been extensively studied. Herein, we compared models using clinical, primary tumor, and metastatic features to estimate cancer-specific survival (CSS) for patients with m-ccRCC Methods: We studied 266 patients undergoing nephrectomy from 1970 to 2019 who had a single site of m-ccRCC completely resected. Select features were used to calculate two versions of the m-ccRCC score published by Leibovich et al. in 2005: one using grade and necrosis from the primary tumor, as originally reported, and one using grade and necrosis from the metastasis. The predictive ability of these two versions of the Leibovich m-ccRCC score, as well as a third model with metastatic features only (site, timing in relation to nephrectomy, grade, coagulative tumor necrosis, and sarcomatoid differentiation), were compared using c-indexes from Cox proportional hazards regression models Results: Clinical, primary tumor, and metastatic features are shown in Table 1. A total of 197 patients died from RCC at a median of 2.3 years (IQR 1.1-4.5) with a median follow-up for survivors of 13.2 years (IQR 10.0-14.5). Model performance is summarized in Table 2. The Leibovich score calculated using grade and necrosis from the metastasis had similar predictive ability compared to the original score calculated using grade and necrosis from the primary tumor. A third model demonstrated that metastasectomy at the time of or within 2 years after nephrectomy, bone metastasis, advanced grade, and sarcomatoid differentiation in the metastatic tumor were significantly associated with death from RCC Conclusions: The Leibovich scoring algorithm, calculated with either primary or metastatic histopathology, can be used to estimate CSS for patients with m-ccRCC. These findings are of particular importance for instances when the primary tumor pathology is not readily available SOURCE OF Funding: none