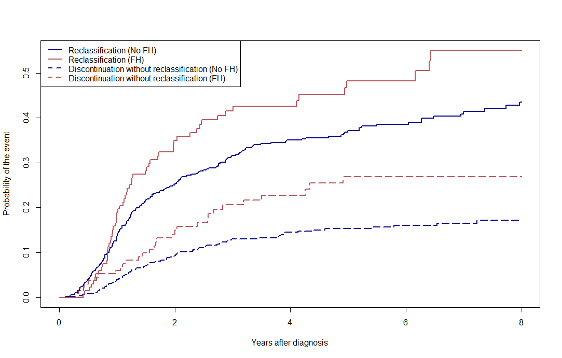
Introduction: Men with family history (FH) of prostate cancer (PCa) on active surveillance (AS) for low grade PCa are at higher risk of reclassification. In these patients, however, adherence to AS may be influenced by factors other than reclassification. We assessed the relationship between FH and AS drop-out without evidence of reclassification compared to patients without FH. Methods: We identified 779 men on AS for grade group 1 or 2 PCa at our Institution (2005-2021). Reclassification was defined as an increase in Gleason score from diagnosis. The cumulative incidence function estimated the 5-year discontinuation rate without reclassification according to FH (any-degree, vs no FH), with discontinuation for reclassification as a competing event. The Fine and Gray model was used to derive the adjusted sub-distribution hazard ratios (aSHR). A sensitivity analysis was conducted incorporating a definition of volume reclassification (>33% of cores involved or >50% of a single core involved), and the NCCN definition of strong FH (=1 first-degree or =2 second-degree relatives). To assess clinical utility, we evaluated rates of adverse pathology ([AP], grade group =2, extracapsular extension, or positive lymph nodes) in 246 men who underwent delayed radical prostatectomy (RP) according to the reason for discontinuation. Results: Median age was 65 years (59-70 yrs), 135 men (18%) had FH, and 112 (14%) had strong FH. Median follow-up was 50 months, the overall 5-year reclassification rate was 42%. The overall 5-year rate of discontinuation without reclassification was 23% (n=118). The cumulative incidence of 5-year discontinuation without reclassification in patients with, vs without FH was 27% vs 15% (aSHR 1.61, p=0.029). The effect of FH on discontinuation without reclassification remained significant in all sensitivity analyses. No difference was observed in terms of AP at delayed RP according to FH in those reclassified vs those treated without reclassification (all p>0.05). Conclusions: Although FH is associated with higher risk of reclassification, almost a third of men with positive FH discontinue AS without evidence of progression. The absence of a difference in AP rates at delayed RP should guide patient counseling about safety of AS also in men with FH. SOURCE OF Funding: .

 photo")