Session: MP78: Trauma/Reconstruction/Diversion: Urethral Reconstruction (including Stricture & Diverticulum) II
MP78-09: Salvage Direct Vision Internal Urethrotomy for After Failed Substitution Urethroplasty: Extended Long-term Follow-up From a Reconstructive Referral Center
Brigham and Women's Division of Urological Surgery and Center for Surgery and Public Health
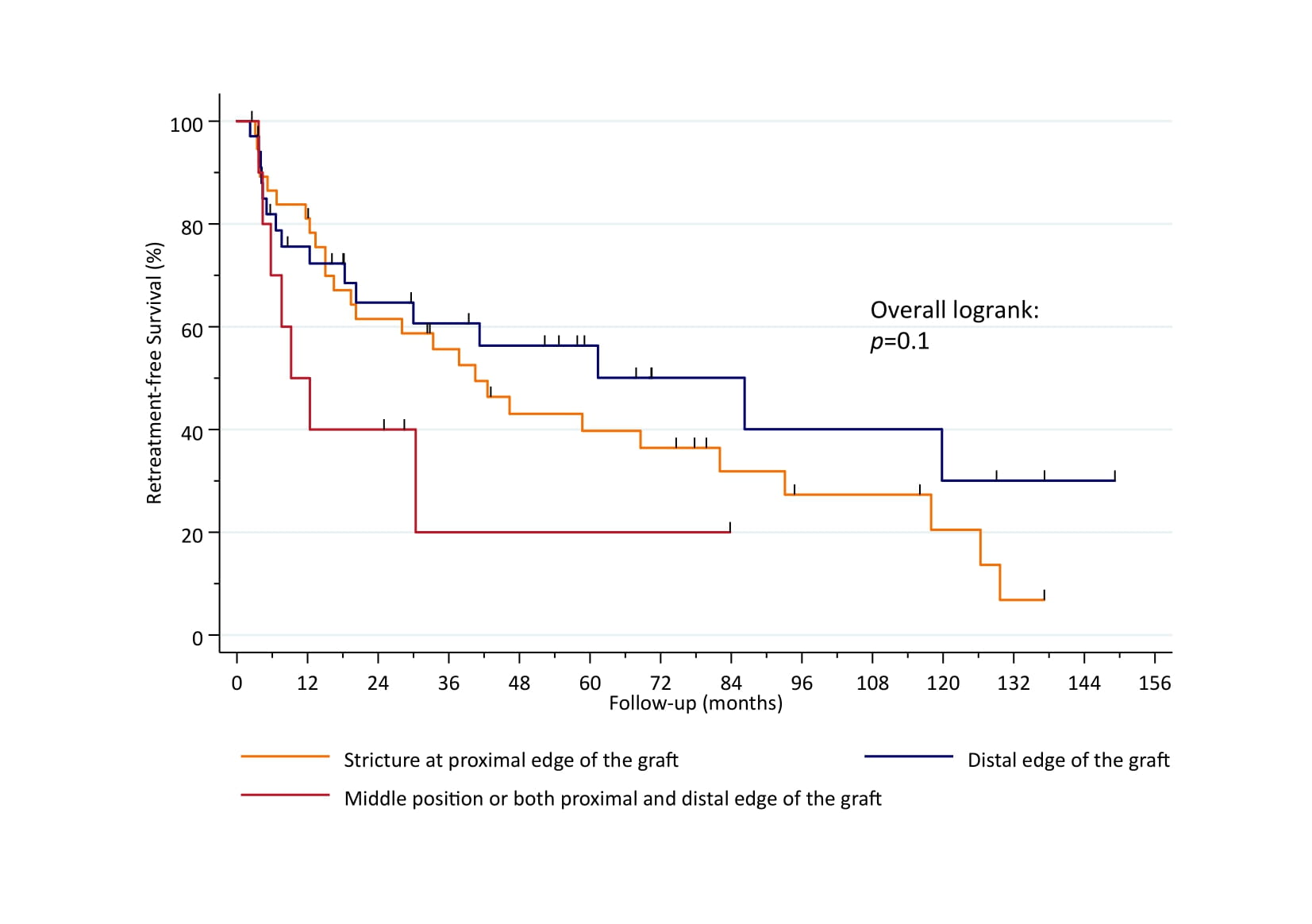
Introduction: There is controversy regarding the optimal salvage treatment option for stricture recurrence after anterior buccal mucosal graft urethroplasty (BMGU). Data on retreatment modalities and their outcomes are scarce. Thus, we aimed to report on our extended follow-up of patients undergoing direct vision internal urethrotomy (DVIU) for short, veil-like recurrences after anterior BMGU. Methods: We included all men undergoing salvage DVIU for recurrence with short segment, anastomotic fibrous rings after prior BMGU at our center between 2009-2021. We recorded clinical characteristics such as stricture location relative to the buccal graft (proximal, middle, distal), time from BMGU to DVIU in months, and etiology. Primary endpoint was retreatment-free survival after salvage DVIU. Kaplan-Meier analysis was performed for censoring and subsequent treatment modalities in the case of recurrence after salvage DVIU were extracted. Results: Overall, 105 patients underwent DVIU after BMGU for bulbar (66%), penobulbar (16%), penile (15%), or membranous stricture (2.9%). 45% of strictures were proximal of the graft, 43% distal, and 12% were located in a middle position or both proximal and distal of the graft. The majority of strictures were iatrogenic (67%), followed by idiopathic (13%), inflammatory (9.6%), and posttraumatic etiology (7.7%). Median time from BMGU to salvage DVIU was 10 mo (IQR 4.2-28). 13 men (12%) were lost to follow-up and at a median follow-up of 74 mo (IQR 32-127), 53 men (58%) suffered from stricture recurrence (median time to recurrence: 15 mo [IQR 5.0-41]). 12-mo retreatment-free survival was 86%, 82%, and 70% for proximal, distal, and middle/both proximal + distal stricture position, respectively (p=0.1; Figure 1). In patients recurring after salvage DVIU, most subsequent interventions consisted of redo BMGU (46%) and redo salvage DVIU (31%). Conclusions: Salvage DVIU for veil-like, short segment recurrences remains a limited but viable endoscopic treatment option after anterior BMGU. Pending larger multi-institutional validation, the benefit of DVIU appears more pronounced for anastomotic rings developing at the distal edge of the buccal graft. SOURCE OF Funding: n/a