
.png)
Case Series/Study
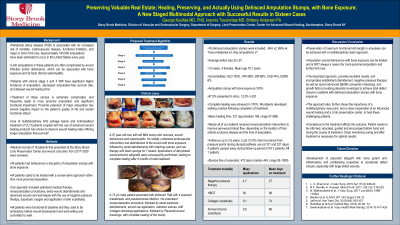
Limb amputations in patients with severe peripheral arterial disease are frequently complicated by wound infection and/or dehiscence. These cases are frequently associated with bone exposure and de facto clinical osteomyelitis. Treatment of these stumps is frequently associated with eventual more proximal amputation and significant functional impairment.
We describe here our experience of healing 16 of these cases, using a combination of established and new advanced techniques, in a staged approach, designed to address all sequential aspects and phases of wound closure.
Methods:
16 dehisced amputation stumps were included.3 above, 6 bellow knee, 5 trans metatarsal, and 2 Ray amputations. All had bone exposure. Average defect size was 58cm2.
All were treated with a 5-stage approach :
Stage 1: PICC Line insertion - antibiotics, aggressive endovascular revascularization to maximize arterial perfusion, in ALL patients
Stage 2: Operative removal of non-viable tissues
Stage3: Serial debridements, retention sutures to decrease defect size, and negative pressure therapy. Collagen dressings to prevent biofilm reformation.
Stage 4: When granulation present, Application of amniotic membrane allograft dressings.
Stage 5: Re fitting of the stump and initiation and walking trials.
Results:
There was no mortality. ALL 16 patients healed, with NO proximal extension of amputation.
ALL patients-initiated physical therapy and walking routines after stump/prosthesis fitting.
The mean--entire group- healing time, including the patients with large defects, was 218 days i.e. 7.7months. 2 out of the 16 patients, have had a recurrence from pressure points during stump/prosthesis use.
Discussion:
Preservation of the maximum possible functional limb length is crucial for patient’s ambulation and quality of life.
This newly described approach, provides excellent results, and incorporates established (debridement, negative pressure therapy) as well as recent advanced (Biofilm reformation prevention collagen dressings, and dehydrated placental coverings) to achieve total defect closure in patients with dehisced amputation stumps with bone exposure.
This approach also, further shows the importance of a multidisciplinary view point, and a close cooperation of an Advanced wound healing and a Limb preservation center, to heal these challenging patients.
Trademarked Items:
References: