
.png)
Health Economics
The prevalence of diabetes exceeds 10% of the US population with calculated annual costs of $327 billion in 2017 and increasing. Additionally, lower extremity diabetic ulcers (LEDU) present a substantial financial and disutility burden to both the patient and payor. Patients with LEDUs face challenges with mobility, infections, amputations and shortened lifespan. This analysis evaluated the cost-effectiveness and budget impact of using standard care (No Advanced Treatment, NAT) compared to an Advanced Treatment (AT), Dehydrated Amnion/Chorion Membrane (DHACM) allografts, particularly when AT was initiated following parameters for use (FPFU) (starting within 30–45 days of diagnosis and applied every 7–14 days).
A retrospective analysis of Medicare data files from 2015-2019 was the basis for four propensity-matched cohorts of LEDU episodes. Outcomes for DHACM and NAT including amputations, and healthcare utilization were analyzed from claims to build a hybrid economic model, combining a one-year decision tree and a four-year Markov model using a healthcare sector perspective. The budget impact was evaluated in the difference in per member per month spending following completion of the decision tree. Cost-effectiveness was analyzed before and after the Markov model at a willingness-to-pay threshold of $100,000 per quality adjusted life year (QALY).
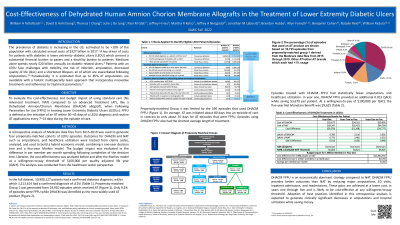
There were 10,900,127 patients with a diagnosis of diabetes, of whom 1,213,614 had a LEDU. Propensity-matched Group 1 was limited to the 19,910 episodes which received AT. DHACM was identified as the most widely used AT product and propensity-matched Group 4 was limited to the 590 episodes that used DHACM FPFU. Only 9.2% of episodes were FPFU. Episodes treated with DHACM FPFU had statistically fewer amputations and healthcare utilization. In year one, DHACM FPFU provided an additional 0.013 QALYs while saving $3,670 per patient. At a willingness-to-pay of $100,000 per QALY, the five-year Net Monetary Benefit was $9,625.
DHACM FPFU is an economically dominant strategy compared to NAT, reducing major amputations, ED visits, inpatient admissions, and readmissions. These calculated gains were achieved at a lower cost, in years one through five and was likely to be cost-effective at any willingness-to-pay threshold. Further education on and adoption of the best practices identified in this analysis could potentially have a favorable long-term impact on clinical outcomes while concurrently reducing medical expenditures.