(CS-126) Use of Negative Pressure Wound Therapy in Patients with Complex Abdominal Wounds with Enterocutaneous Fistula
Co-Author(s):
Diane Wagner, MSN, CWOCN – Temple University Hospital
Introduction: Complex wounds can be difficult to heal and may require advanced wound care techniques. In some patients, wound healing can be further complicated by the presence of an enterocutaneous fistula (ECFs) and the associated effluent. ECF effluent is corrosive, and the continuous moisture can damage surrounding skin and increase the risk for infection.1 In patients with ECFs requiring wound care, the fistula and associated effluent is isolated from the wound bed prior to the initiation of wound care. The use of negative pressure wound therapy (NPWT) for wound management in patients with abdominal wounds with ECFs is assessed.
Methods: Antibiotics were initiated as needed and surgical wound debridement was performed if required. Ostomy paste or barrier seal was used to protect periwound skin. Non-adherent silicone dressings* were used to protect delicate structures. Any fistulas in the wound bed were isolated prior to application of NPWT†. Non-adherent silicone dressings or calcium alginate dressings were used to protect the fistulas. Ostomy appliances were employed to contain fistula effluent away from the wound bed. NPWT dressings were changed every 2-3 days.
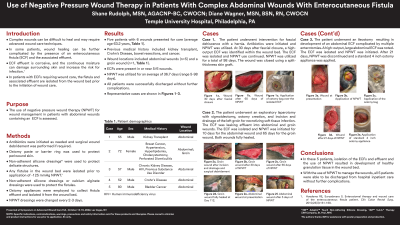
Results: Five patients with 6 wounds presented for care (average age 63.2 years). Previous medical history included kidney transplant, Crohn’s disease, bowel resections, and cancer. Wound types included abdominal wounds (n=5) and a groin wound (n=1). Enterocutaneous fistulas were present in or near 5/6 wounds. NPWT was utilized for an average of 36.7 days (range 5-98 days). Development of healthy granulation tissue was observed in wounds with the use NPWT. All patients were successfully discharged without further complications.
Discussion: In these 5 patients, isolation of enterocutaneous fistulas and fistula effluent and use of NPWT resulted in development of healthy granulation tissue in the wound bed. With the use of NPWT to manage the wounds, all 5 patients were able to be discharged from hospital inpatient care without further complications.
References: 1. Hoedema RE, Suryadevara S. Enterostomal therapy and wound care of the enterocutaneous fistula patient. Clin Colon Rectal Surg. 2010;23(3):161-168.

.png)