(CS-039) Simplifying the reconstruction of soft tissue defects following extirpative procedures for cutaneous malignancies using a decellularized fish skin graft*
Co-Author(s):
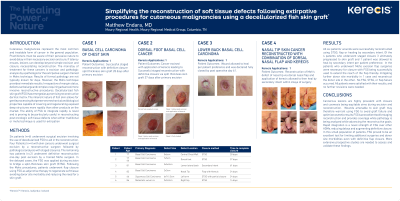
<b>Introduction</b>: <p class="MsoNormal"><span style="font-family: 'Times New Roman',serif;">Cutaneous malignancies represent the most common and treatable form of cancer in the general population. Practitioners must be aware of their pervasive nature to avoid delay in their necessary excision and cure. If latency ensues, lesions can develop beyond simple excision and closure, necessitating reconstruction. Decellularized fish skin graft* (FSG) has emerged as a promising reconstructive dermal matrix. The nature of fish skin allows for gentle processing preserving mechanical and biological properties capable of covering and regenerating exposed deep structures. The ability of FSG to integrate rapidly is proving to be particularly useful in reconstructing post oncologic soft tissue defects.</span></p><br/><br/><b>Methods</b>: <p class="MsoNormal"><span style="font-family: 'Times New Roman',serif;">Six patients (n=6) underwent surgical excision involving the use of decellularized FSG to aid in the reconstruction. Four Patients (n=4) with skin cancers underwent surgical excision by a reconstructive surgeon followed by pathological analysis with staged closures. The remaining two patients (n=2) underwent definitive reconstruction one-day post excision by a trained Mohs surgeon. In the delayed cases, the FSG was applied during excision to bridge a split-thickness skin graft (STSG). Following the Mohs procedures, patients underwent flap closure using FSG as adjunctive therapy to regenerate soft tissue avoiding donor site morbidity and reducing the need for a skin graft. </span></p><br/><br/><b>Results</b>: <p class="MsoNormal"><span style="font-family: 'Times New Roman',serif;">All six patients' wounds were successfully reconstructed using STSG, flap or healing by secondary intent. Of the 4 patients who underwent staged closure 3 ultimately progressed to skin graft and 1 patient healed by secondary intent per patient preference.<span style="mso-spacerun: yes;"> </span>In the patients who underwent Mohs excision, flap surgeries were necessary for closure with FSG being used to extend the reach of the flap mitigating further donor site morbidity in 1 case and reconstruct the donor site in the other.<span style="mso-spacerun: yes;"> </span>No FSG, STSG, or flap failure occurred. All patients were satisfied with their results, and no further revisions were needed.</span></p><br/><br/><b>Discussion</b>: <p class="MsoNormal"><span style="font-family: 'Times New Roman',serif;">Cancerous lesions are highly prevalent with closure and cosmesis being equitable aims during excision and reconstruction.<span style="mso-spacerun: yes;"> </span>Wounds amenable to skin graft may warrant using FSG to avoid graft failure and optimize cosmetic results. FSG is an excellent tool for staging reconstruction and provides coverage while advancing the reconstructive goals. Rapid integration is a novel strength of FSG over other ADMs, reducing delays and augmenting definitive closure. In this population of patients, FSG proved to be an excellent tool for limiting additional surgeries and donor site morbidities. More extensive prospective studies are needed to assess and validate these findings.</span></p><br/><br/><b>Trademarked Items</b>: *KerecisTM<br/><br/><b>References</b>: <br/><br/>

.png)