(CS-056) Recalcitrant wounds successfully treated in skilled nursing facilities using a novel omega fatty acid treatment protocol
Co-Author(s):
Tiffany Forquer, PA-C – Skin & Wound Specialist, United Wound Healing; Danae Kissner, PA-C – Skin & Wound Specialist, United Wound Healing; Shavonne Tonnes, PA-C – Skin & Wound Specialist, United Wound Healing; Rachel Westman, APRN, AGPCNP-C – Skin&Wound Care Specialist, United Wound Healing; Brianna Primrose, ARNP – Skin & Wound Specialist, United Wound Healing
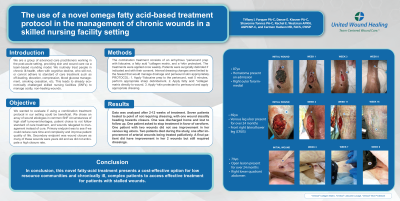
<b>Introduction</b>: <p class="MsoNormal">We are a group of advanced care practitioners working in the post-acute setting, providing skin and wound care via a team-based rounding model. We routinely treat people in chronic ill-health, often with cognitive decline, who will not, or cannot adhere to standard of care treatment such as off-loading, elevation, compression, blood glucose management, smoking cessation, etc. This leads to already economically challenged skilled nursing facilities (SNFs) to manage costly, non-healing wounds.</p> <p class="MsoNormal">Omeza’s novel treatment is less costly and easier to apply than many advanced therapies; characteristics that are crucial for the SNF setting.</p><br/><br/><b>Methods</b>: <p class="MsoNormal">We wanted to evaluate if using a combination treatment protocol in our setting could be beneficial. We chose an array of wound etiologies in common SNF circumstances of high staff turnover/shortages, patient choice to not follow standard of care treatment, and wounds relegated to management instead of cure. Primary endpoint was to see if we could reduce care time and complexity and improve patient quality of life. Secondary endpoint was wound closure as many of these wounds were years old and we did not anticipate a high closure rate.</p> <p class="MsoNormal">The combination treatment consists of Omeza® lidocaine lavage, Omeza® collagen matrix, and Omeza® skin protectant. The treatments were applied once weekly. Patients were surgically debrided if indicated and with their consent. Interval dressing changes were limited to the fewest that would manage drainage and periwound skin appropriately.</p><br/><br/><b>Results</b>: <span style="font-size: 11.0pt; line-height: 107%; font-family: 'Calibri',sans-serif; mso-ascii-theme-font: minor-latin; mso-fareast-font-family: Calibri; mso-fareast-theme-font: minor-latin; mso-hansi-theme-font: minor-latin; mso-bidi-font-family: 'Times New Roman'; mso-bidi-theme-font: minor-bidi; mso-ansi-language: EN-US; mso-fareast-language: EN-US; mso-bidi-language: AR-SA;">Data was analyzed after 2-12 weeks of treatment. Two patients died during the study, one after improvement of arterial wounds being treated palliatively. One patient asked to stop treatment in favor of xeroform. One was discharged home and lost to follow up. Seven patients healed to point of not requiring dressings, with one wound steadily heading towards closure. One patient with two wounds did not see improvement in her venous leg ulcers. A final patient did have improvement in her 2 wounds but still required dressings.</span><br/><br/><b>Discussion</b>: <p class="MsoNormal">In conclusion, Omeza’s novel treatment presents a cost-effective option for low resource communities and chronically ill, complex patients to access effective treatment for patients with stalled wounds.</p><br/><br/><b>Trademarked Items</b>: Omeza® lidocaine lavage, Omeza® collagen matrix, and Omeza® skin protectant<br/><br/><b>References</b>: <br/><br/>

.png)