(PI-015) Development of a soft tissue reconstructive ladder in trauma patients to improve patient and health care outcomes with the use of negative pressure wound therapy systems and cellular tissue products.
Co-Author(s):
Esther Kim, DO – Surgery Resident, Tower Health System; Amanda McNicholas, DNP, MBA, CRNP – Chief Advanced Practice Provider Officer, Trauma Surgery, Tower Health System
Introduction: Soft tissue injuries most commonly result from an infectious cause, such as necrotizing soft tissue infection or via traumatic injury. While each patient has unique needs based upon their history and the anatomical location and nature of injury, care for these patients is often multidisciplinary involving the trauma surgical team, CWOCN team, plastic surgery team, physical and occupational therapy, and case management. It was identified that the projected treatment guidelines were ill-defined in a Level 1 Trauma Center in Eastern, Pennsylvania. The providers and clinicians had little to no guidance for timing of advanced therapies such as negative pressure wound therapy (NPWT*), negative pressure wound therapy with instillation and dwell (NPWTi-d†), and use of grafting. The length of stay for this patient population is often weeks to months in the acute care setting.
Methods: A literature review was performed that identified there is a dearth of literature to drive the timing of advanced interventions. There were separate guidelines for treatment of infection in skin and soft tissue infections, chronic wounds, and crush injuries. Soft tissue injuries, admitted to the trauma center for three months prior, were reviewed. The treatment plan, clinical course, and discharge status were reviewed. Similarities and differences in the clinical course were examined in further detail.
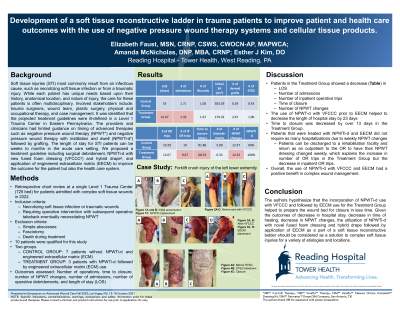
Results: It was found that the trauma team always included surgical debridement. Some wounds were treated with packing, and others treated with either NPWT, or some with NPWTi-d. No cellular tissue products were applied prior to split-thickness skin graft (STSG) application. A treatment plan was implemented for any patient admitted with soft tissue injury. This included wide excisional debridement of non-viable tissue in the operating room (OR), application of NPWTi-d with a fused foam dressing‡ and hybrid silicone acrylic drape§ until no further debridement was required, application of dermal matrix with NPWT as a bolster, and finally STSG or secondary closure by re-epithelization. To date, 3 patients have been treated using these guidelines.
Discussion: The use of the treatment guidelines for soft tissue injury reduced length of stay, OR visits, and number of NPWT and/or NPWTi-d application/ kits used. It is hypothesized that this will reduce cost of care to the health system and overall costs of care. All the patients treated with the new guidelines had favorable wound outcomes without readmission for wound complications. Adoption of these guidelines and further clinical correlations should be researched in the future.
References: 1. Eriksson, E., Liu, P. Y., Schultz, G. S., Martins-Green, M. M., Tanaka, R., Weir, D., Gould, L. J., Armstrong, D. G., Gibbons, G. W., Wolcott, R., Olutoye, O. O., Kirsner, R. S., & Gurtner, G. C. (2022). Chronic wounds: Treatment consensus. Wound Repair and Regeneration, 30(2), 156-171. https://doi.org/10.1111/wrr.12994 2. Sartelli, et. al. (2022). WSES/ GAIS/ WSIS/ SIS-E/ AAST global clinical pathways for patients with skin and soft tissue infections. 3. Krost. (2008). Beyond the Basics: Crush Injuries and Compartment Syndrome. EMS Magazine., 37(2), 67–71. https://doi.org/info:doi/

.png)