
.png)
Case Series/Study
Pyoderma gangrenosum is clinically defined as neutrophilic noninfectious dermatosis. It is a rare, but serious ulcerative disease that has multiple manifestations (1). It was first described in 1916 by Brocq as “phagédenisme géométrique” and the term pyoderma gangrenosum was later coined in 1930 by Brunsting, Goeckerman and O’Leary (2). It often occurs with systemic disease such as rheumatoid arthritis, inflammatory bowel disease, hepatopathies, and other immunological disorders. Initial manifestations of pyoderma gangrenosum (PG) were identified as skin ulcerations with purulent or fluctuant nodules (3). However, the classical representation is described as ulcer with boggy or necrotic wound base with raised inflammatory border (2, 3). PG has several manifestations but it is most commonly seen in lower extremities, commonly along the pretibial region (1,3). PG is said to have an incidence rate of 3-5 in million (1,5), however the true prevalence of PG is not well documented due to failure to diagnose (4). It commonly occurs in adults between the ages of 30-50, predominantly female (3,4,5). Even with low incidence, there are several treatments for treating PG such as steroids, immunosuppressants, immune modulation and anti-inflammatory. In this study, we use Kerecis to treat chronic lower extremity ulcer. This case study, we present an alternate treatment for PG ulceration without the need for serial debridements, as studies have shown debridement of PG ulcers can lead to poor outcomes (6).
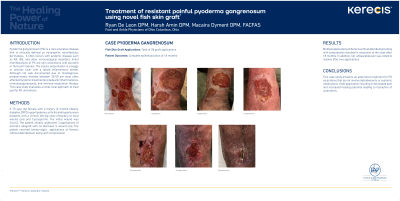
Methods: Patient is a 70-year-old female with history of morbid obesity, chronic regional pain syndrome, hyperlipidemia, arthritis, GERD, hypokalemia, vitamin D deficiency, and hypertension with left leg ulcer present since May, 2020. Dermatology prescribed Cyclosporine for the patient. The initial wounds were 34, 8 and 1 square centimeters. Patient initially underwent 3 applications of amniotic allograft without improvement in wound size.
Results: Multiple applications of Kerecis allograft without debridement of ulcer along with compression over the course of 2 years finally led to resolutions of multiple lower extremity ulcerations. It was also noted that her unbearable pain greatly subsided after four applications.
Discussion:
Trademarked Items: *KerecisTM, Kerecis, Isafjordur, Iceland
References: 1. Brooklyn T, Dunnill G, Probert C. Diagnosis and treatment of pyoderma gangrenosum BMJ 2006; 333 :181
2. Ruocco, E., Sangiuliano, S., Gravina, A., Miranda, A. and Nicoletti, G. (2009), Pyoderma gangrenosum: an updated review. Journal of the European Academy of Dermatology and Venereology, 23: 1008-1017.
3. Neil Crowson, A., C. Mihm Jr, M. and Magro, C. (2003), Pyoderma gangrenosum: a review. Journal of Cutaneous Pathology, 30: 97-107.
4. Frank C Powell, Sinead Collins,Pyoderma gangrenosum, Clinics in Dermatology, Volume 18, Issue 3, 2000, Pages 283-293,
5. Powell FC, Su WPD, Perry HO. Pyoderma gangrenosum: classification and management. J Am Acad Dermatol 1996; 34: 395.
6. David L Steed, Debridement; The American Journal of Surgery, Volume 187, Issue 5, Supplement 1,2004, Pages S71-S74