
.png)
Case Series/Study
Necrotizing infections are complex situations. The incidence of necrotizing fasciitis in diabetics is as high as 40%-60%1, with initial mortality rates of 15%-35%.2,3
Xenogenic skin graft substitutes are applied wounds to enhance the environment, replace dermis, and minimize wound contraction. Piscine acellular dermal matrix* grafts have a native dermal structural, porosity and biomechanical properties that favors cell ingrowth and provides a bacterial barrier with Omega3 fatty acids, which assist the wound in leaving the chronic inflammatory state.6 We illustrate a case where piscine ADM was utilized to reconstruct the soft tissue in a patient with necrotizing fasciitis for limb salvage.
Methods:
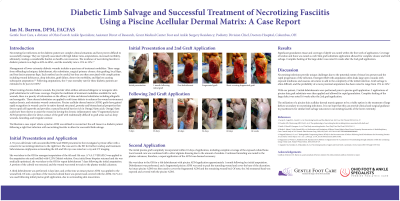
We illustrate a case report where a piscine acellar dermal matrix was utilized for reconstruction and salvage in a diabetic patient with necrotizing fasciitis. With our patient, 2 initial debridements were performed prior to piscine graft application. 2 applications of piscine skin graft substitute were then applied and allowed for rapid granulation.
Results:
Significant granulation tissue and coverage of depth was noted within the first week of application. Coverage of tendon and bone was noted as well. Skin graft substitute application allowed for complete closure and limb salvage. Complete healing of the large defect was noted 16 weeks after the 2nd graft application.
Discussion:
Necrotizing infections provide unique challenges due to the potential extent of tissue loss present and the rapid progression of the infection. Limb salvage is often difficult, and the probability of a more proximal amputation has been noted to range from 15% to 24%.
The utilization of a piscine skin acellular dermal matrix appears to be a viable option in the treatment of large defects secondary to necrotizing infections to aid in limb salvage. It is our hope this can provide clinical and surgical guidance to practitioners for similar limb salvage outcomes in necrotizing fasciitis of the lower extremity.
Trademarked Items: *KerecisTM, Kerecis, Isafjordur, Iceland
References: 1. Iacopi E, Coppelli A, Goretti C, et al. Necrotizing fasciitis and the diabetic foot. Int J Low Extr Wound 2015;14:316–27.
2. Dworkin MS, Westercamp MD, Park L, et al. The epidemiology of necrotizing fasciitis including factors associated with death and
3. Smith J, Horrall S, Juergens A, et al. Total body necrotizing fasciitis. Proc (Bayl Univ Med Cent) 2019;32:61–2.
4. Shakir S, Messa CA 4th, Broach RB, et al. Indications and Limitations of Bilayer Wound Matrix-Based Lower Extremity Reconstruction: A Multidisciplinary Case-Control Study of 191 Wounds. Plast Reconstr Surg. 2020;145(3):813–822. doi:10.1097/PRS.0000000000006609
5. Wagstaff, Marcus J.d., et al. “Biodegradable Temporising Matrix (BTM) for the Reconstruction of Defects Following Serial Debridement for Necrotising Fasciitis: A Case Series.” Burns Open, vol. 3, no. 1, 2019, pp. 12–30., doi:10.1016/j.burnso.2018.10.002.
6. Magnusson S, Winters C, Baldursson BT, Kjartansson H, Rolfsson O, Sigurjonsson GF. Acceleration of wound healing through utilization of fish skin containing omega-3 fatty acids. Today’s Wound Clinic. 2016;10(5):26–29.
7. Angoules AG, Kontakis G, Drakoulakis E, et al. Necrotising fasciitis of upper and lower limb: a systematic review. Injury 2007; 38 Suppl 5:S19–S26.