JL1010E: Efficacy and safety of teclistamab (tec), a B-cell maturation antigen (BCMA) x CD3 bispecific antibody, in patients (pts) with relapsed/refractory multiple myeloma (RRMM) after exposure to other BCMA-targeted agents
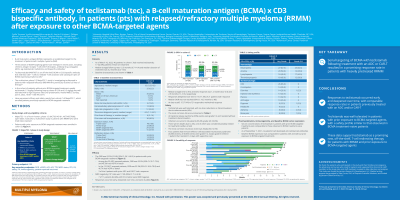
Background: Tec (JNJ-64007957) is a BCMA x CD3 bispecific antibody (Ab) that redirects CD3+ T cells to mediate T-cell activation and subsequent lysis of BCMA-expressing myeloma cells. MajesTEC-1 is a multicohort, open-label phase 1/2 study of tec in pts with RRMM who previously received ≥3 prior lines of therapy (LOT). Results from a pooled analysis of phase 1 and phase 2 cohort A (median follow-up 7.8 mo) demonstrated an overall response rate (ORR) of 62.0% in pts with no prior anti-BCMA treatment (tx). We present initial results from cohort C, in which pts had prior exposure to an anti-BCMA tx.
Methods: Eligible pts (age ≥18 y) had documented MM per IMWG criteria and had received ≥3 prior LOT including a PI, an IMiD, an anti-CD38 Ab, and an anti-BCMA tx (chimeric antigen receptor T [CAR-T] or Ab drug conjugate [ADC]). Pts were enrolled into a Simon’s stage design, receiving weekly subcutaneous tec 1.5 mg/kg preceded by step-up doses of 0.06 and 0.3 mg/kg. Primary endpoint was ORR (per IMWG 2016 criteria). AEs were graded per CTCAE v4.03; cytokine release syndrome (CRS) and immune effector cell–associated neurotoxicity syndrome (ICANS) were graded per ASTCT guidelines.
Results: As of Sep 7, 2021, 38 pts in cohort C received tec (63% male; median age 63.5 y [range 32–82]; median prior LOT 6 [range 3–14]). 32 (84%) pts were refractory to last LOT; 25 (66%) were refractory to an anti-BCMA tx. Of 25 pts evaluated for efficacy, 16 (64%) had prior ADC, 11 (44%) prior CAR-T (2 pts received both). With median follow-up of 6.9 mo (range 0.7–8.7), ORR was 40% (95% CI 21–61). 5 pts (20%) achieved a complete response or better. The ORR (95% CI) was 38% (15–65) in ADC-exposed pts and 45% (17–77) in CAR-T–exposed pts. Most responses occurred rapidly; 7/25 pts had responses that deepened over time. Median time (range) to first and best response was 1.2 mo (0.2–4.9) and 2.1 mo (1.1–5.7), respectively. Median duration of response was not reached. The safety profile was comparable with that observed in BMCA tx-naive pts, with no new safety concerns. 16 pts (42%; grade 3/4 26%) had infections. Most common AEs (n=38) were CRS (63%; all grade 1/2; median [range] time to CRS onset: 3 d [2–6], duration of CRS: 2 d [1–4]), neutropenia (55%; grade 3/4 50%), thrombocytopenia (42%; grade 3/4 29%), anemia (39%; grade 3/4 29%), and lymphopenia (40%; grade 3/4 37%). One pt had grade 3 ICANS that resolved with supportive care; pt remains on tx. No pts developed anti-tec Abs. Baseline BCMA expression was comparable with that observed in BCMA tx-naive pts. Updated efficacy and safety data will be presented for 40 pts.
Conclusion: Initial results of serial targeting of BCMA with tec following ADC or CAR-T tx suggest a promising ORR with responses occurring early and deepening over time. A well-tolerated safety profile was observed in pts previously treated with anti-BCMA tx.