Nurse Practitioner Gyn Oncology NYU Perlmutter Cancer Center NY, New York, United States
Background: Dostarlimab is a humanized programmed death 1 (PD-1) receptor monoclonal antibody that blocks interaction with the ligands PD-L1 and PD-L2. Dostarlimab is approved as a monotherapy in adult patients (pts) with mismatch repair deficient (dMMR; US) or dMMR/microsatellite-instability high (EU) recurrent or advanced endometrial cancer that has progressed progressing on or following prior treatment with a platinum-containing regimen. GARNET is a phase 1 study assessing antitumor activity and safety of dostarlimab monotherapy in pts with solid tumors.
Methods: Pts with dMMR solid tumors, mismatch repair proficient endometrial cancer, and non-small cell lung cancer that progressed on or after prior therapy received 500 mg of dostarlimab IV every 3 weeks (Q3W) for 4 cycles, then 1000 mg IV every 6 weeks (Q6W) for up to 2 years or until disease progression or discontinuation. Here, we report TRAEs by cycle.
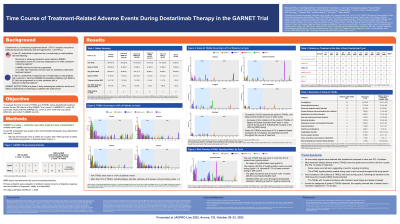
Results: A total of 515 pts were included. Of these pts, 60 (11.7%) experienced TRAEs leading to treatment interruption, and 25 (4.9%) experienced TRAEs leading to discontinuation. TRAEs of any grade with overall incidence of ≥10% of pts are shown (Table 1). The majority of TRAEs occurred during cycles 1–3, with highest incidence during cycle 1. Grade 3 or 4 TRAEs were rare; those seen in ≥1% of pts are shown. Immune-related (ir) TRAEs of any grade with overall incidence of ≥2% of pts are shown. Most cases (96.9%) of irTRAEs occurred during cycles 1–8. The peak incidence of hypothyroidism occurred during cycle 4; in addition, frequency was increased during cycles 5–8, compared with cycles 1–4. No deaths were attributed to dostarlimab.
Conclusions: No new safety signals were detected with dostarlimab compared to other anti–PD-1 inhibitors. Most TRAEs were low grade. The majority of TRAEs and grade ≥3 TRAEs occurred in the first 3 cycles (first 12 weeks), but some cases occurred later, suggesting a need for ongoing monitoring. Few increases in the incidence of TRAEs were seen during cycle 5 following the transition to the 1000-mg Q6W dosing schedule; the TRAEs with increased incidence after the transition were fatigue and lipase increased. An increase in the frequency of the irTRAE hypothyroidism was seen after transitioning to the 1000-mg Q6W schedule.

 photo")