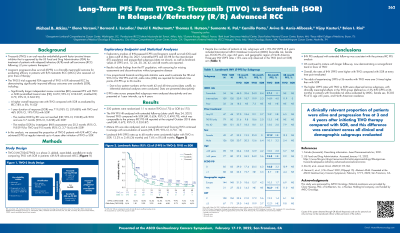
Background: The TIVO-3 trial supported FDA-approval of TIVO in R/R advanced RCC, demonstrating significantly improved PFS over SOR in the primary independent review committee [IRC] analysis (HR: 0.672, 95% CI: 0.52-0.87). Long-term survival without disease progression (LT-PFS) is a clinically meaningful outcome among patients with R/R mRCC and ≥2 lines of prior therapy. We assessed the proportion of TIVO-3 patients living progression-free with R/R mRCC at 6-month intervals up to 4 years post-initiation of TIVO or SOR.
Methods: Exploratory analysis of LT-PFS was calculated using investigator-assessment [INV] with a data cut-off of May 24, 2021. PFS hazard ratio and landmark values of LT-PFS at 6, 12, 18, 24, 30, 36, 42 and 48 months are reported. Results include the ITT population, with censoring for missing assessments and discontinuation without PD. Cox proportional hazards and log-rank statistics were used to estimate the HR and 95% CI for INV-PFS; odds ratios (ORs) are reported for landmark timepoints up to 36-months. LT-PFS across prespecified subgroups were analyzed descriptively.
Results: 350 patients were randomized to TIVO (n=175) or SOR (n=175). INV PFS was superior with TIVO vs SOR (HR: 0.624, 95% CI: 0.49-0.79). Landmark LT-PFS rates up to 48-months are consistently higher with TIVO vs SOR, with 12% vs 2% and 7.6% vs 0% at 3- and 4-years, respectively (Table 1). Despite low numbers of patients at risk with extended follow-up, subgroups with ≥15% LT-PFS at 3-years include IMDC favorable risk, female gender, ECOG PS0, age ≥65 years, and region NA – all confined to the TIVO arm.
Conclusions: INV PFS with long-term follow-up is consistent with primary IRC PFS. Patients treated with TIVO were up to 5X more likely to experience LT-PFS compared to SOR. A clinically relevant minority of patients are alive and progression-free on TIVO at 3- and 4-years.