Introduction: Robot-assisted radical cystectomy (RARC), now widely replacing open surgery (ORC), requires clamping of the ureters which possibly predispose to postrenal acute kidney injury (AKI). We aimed to clarify association between presence and length of ureteral clamping and acute/chronic postoperative kidney function.
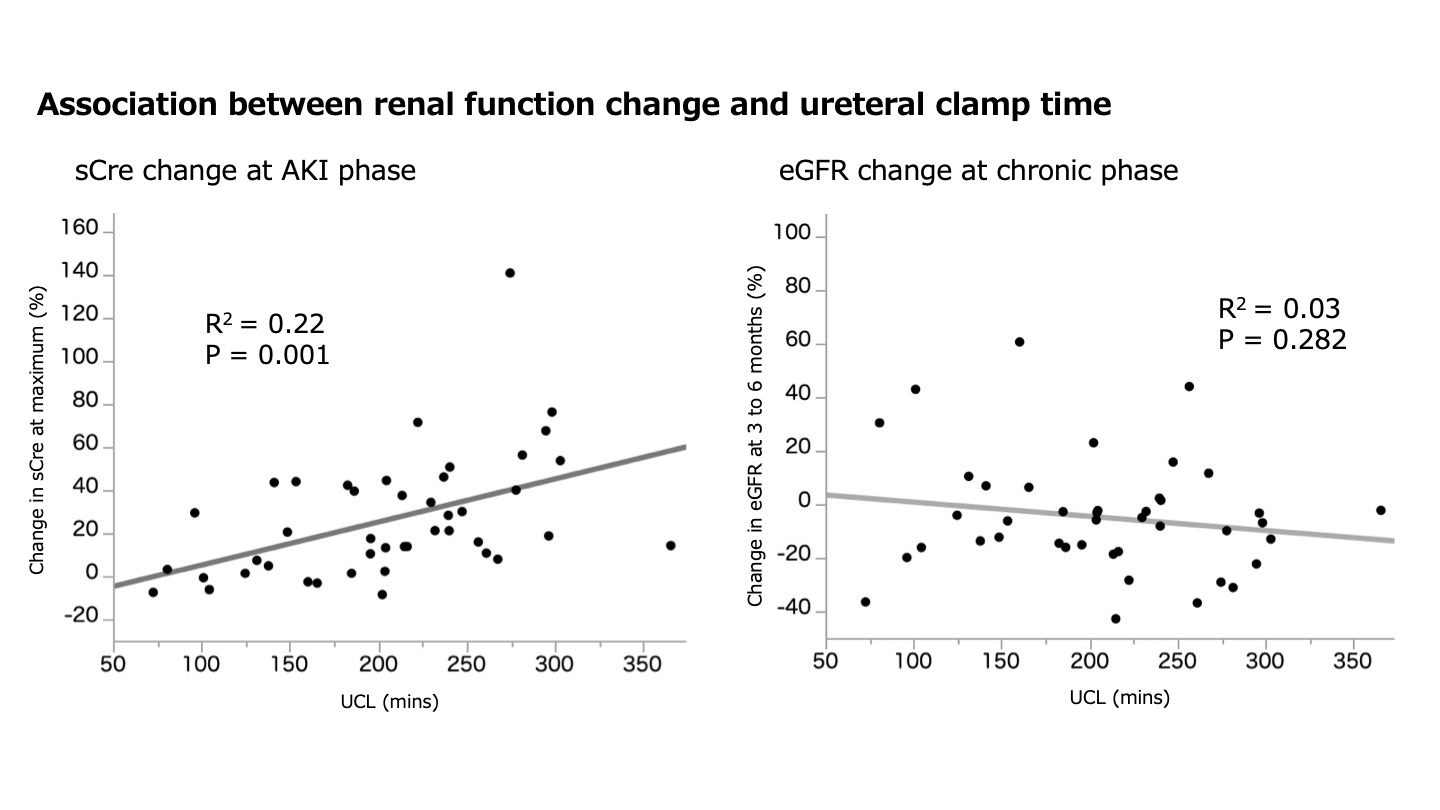
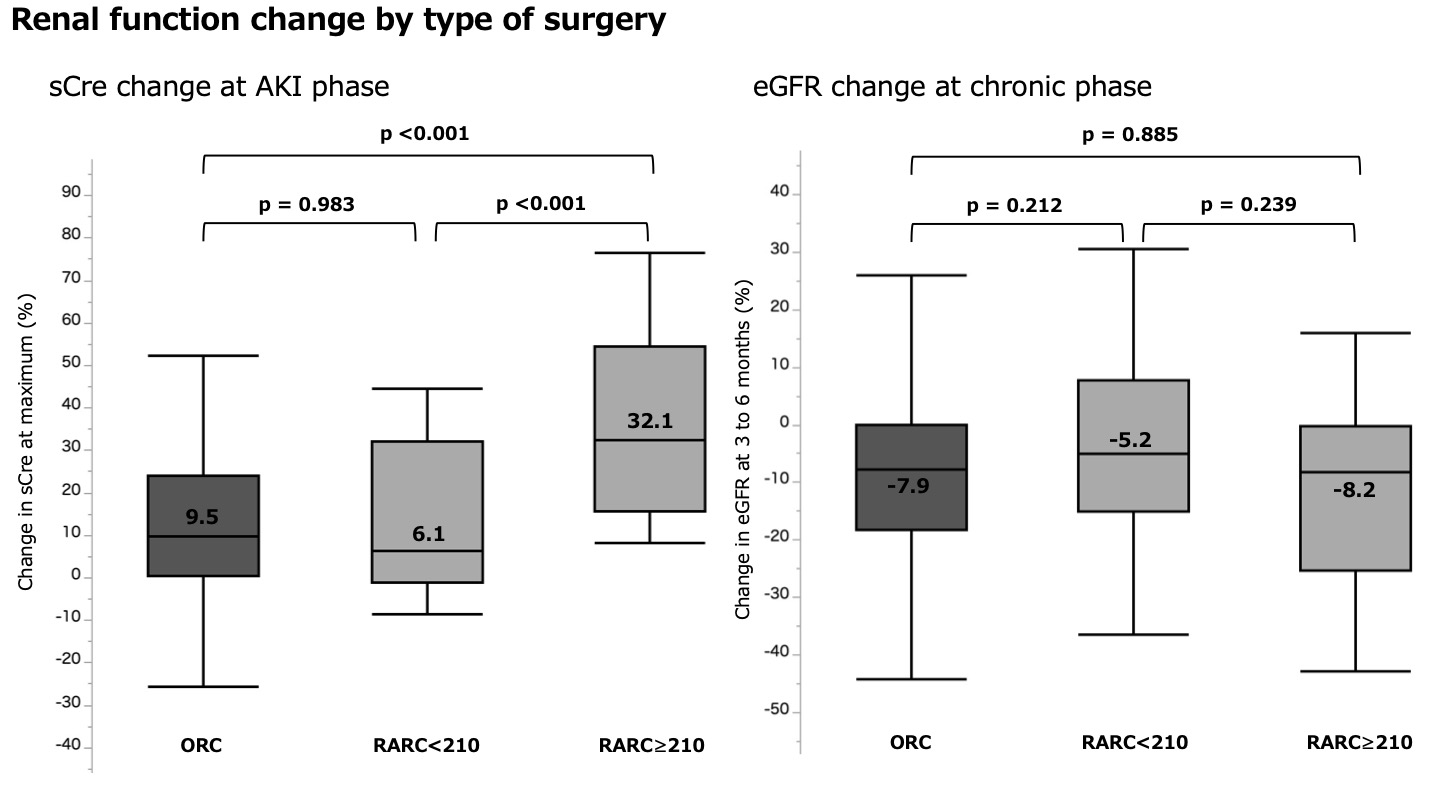
Methods: Patients who underwent radical cystectomy (robotic or open) at two tertiary institutions from 2002 to 2021 were retrospectively enrolled. First, among those underwent robotic RC percentage serum creatinine level change (% sCr change) at its’ maximum after surgery was plotted against length of ureteral clamping to assess their correlation. Furthermore, those patients were grouped into two using a median clamping time (210 min), and the % sCr change at its maximum as well as percentage estimated glomerular filtration rate (% eGFR) change at 3 to 6 months (chronic phase) were compared between three groups, namely RARC <210, RARC=210, and ORC (no clamp).
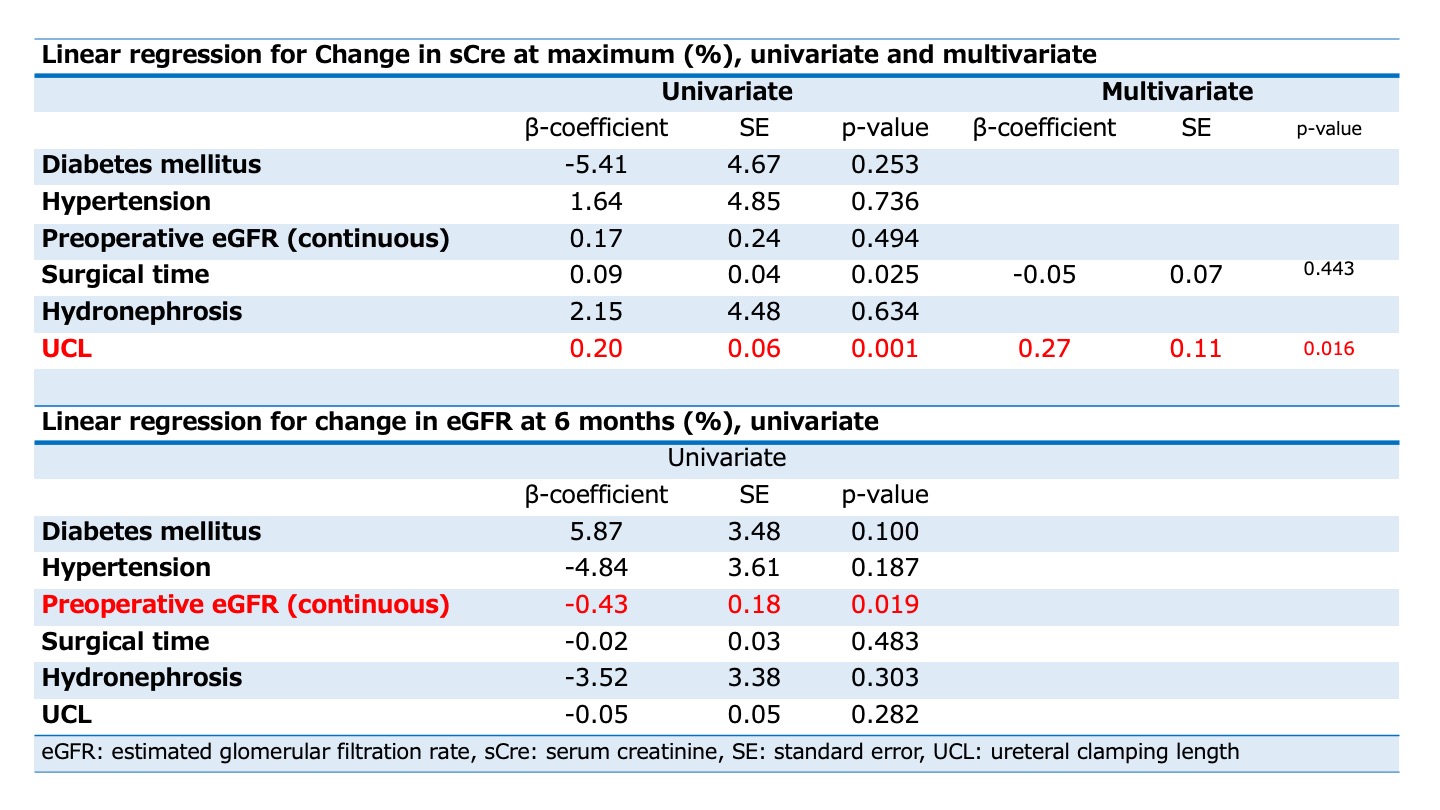
Results: We analyzed 120 patients (44 robotic, 76 open). Weak but significant correlation were observed between length of ureteral clamping and %Cre change (R2=0.22, p=0.001). Across three groups, baseline serum creatinine level were comparable (all, non-significant). % sCr change was significantly larger for RARC=210 (N=17, +32.1) against RARC <210 (N=27, +6.1) or ORC (9.5) (both, p<0.001). Change in chronic % eGFR was comparable across three groups (all, non-significant).
Conclusions: Longer clamping of ureter during RARC may induce AKI. Although impact on chronic renal function were limited, clamping length should be minimized to protect patients from potential harm of AKI.

.jpg)
.jpg)