MP05: Stone Disease: Basic Research & Pathophysiology
MP05-01: Validating the kidney injury test (KIT) as a point of care diagnostic for urinary stone recurrence
Friday, May 13, 2022
8:45 AM – 10:00 AM
Location: Room 225
Xavier Cortez*, San Francisco, CA, Srinka Ghosh, Reuben Sarwal, Nick Titzler, Wanzin Yazar, Brisbane, CA, Marshall Stoller, Minnie Sarwal, Thomas Chi, San Francisco, CA
Introduction: The gold standard to monitor for stone recurrence is imaging, which is inconvenient and costly for patients. This contributes to poor follow-up care for nephrolithiasis patients. A point of care, non-imaging test to monitor for stone growth and recurrence would thus be impactful for patients. The KIT assay measures 4 biomarkers in a spot urine sample. Our lab previously demonstrated that KIT score, a composite of the measured values, accurately demonstrated the presence of calcium-based stones in patients with imaging-proven stones compared to patients without stones. The primary objective of this study was to validate KIT as a method for monitoring stone recurrence and growth by comparing KIT scores over time in a longitudinal cohort of patients.
Methods: Spot urine samples were prospectively collected from stone patients during clinical encounters including routine follow-ups and surgical cases since 2018. A retrospective cohort of patients who provided at least two samples was identified from the Registry for Stones of the Kidneys and Ureter (ReSKU). Samples were found to have corresponding imaging studies within 2 months of each sample collection date to confirm stone presence, absence, or recurrence. Cystinuric patients were excluded. Urine supernatant was assayed for all patients using the KIT assay and KIT scores were calculated.
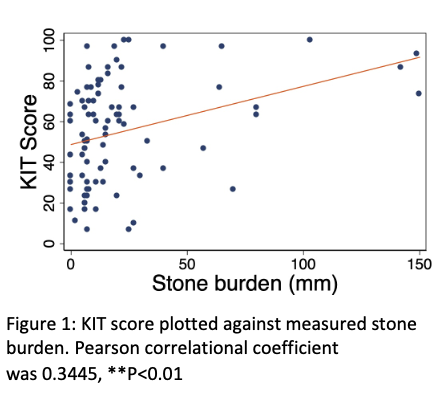
Results: A cohort of 36 patients with 89 samples was analyzed using the KIT assay. 76 samples were collected during stone events. 13 samples were collected during non-stone events. Mean KIT score in patients with active stone events was 57.27 ± 25.52 compared to 41.07 ± 19.97 for non-stone events (p = .018). The Pearson correlational coefficient between stone size and KIT score was 0.3447 (p < .01) [Figure 1]. Nine patients provided at least 1 sample during both a stone and non-stone event for 22 total samples. In a sub analysis of this group, mean KIT score during active stone events was 53.84 ± 21.02 compared to 39.28 ± 19.78 for non-stone events (p = 0.111). Seven of these nine patients underwent a stone procedure prior to providing a sample during a non-stone event.
Conclusions: KIT score can differentiate between stone and non-stone events in nephrolithiasis patients, demonstrating its utility in identifying patients for recurrence in lieu of imaging.

.jpg)
.jpg)