Introduction: Use of fluoroscopy is essential in percutaneous nephrolithotomy (PCNL) but poses potential health risks for patients and operating room staff. Therefore, despite advances in C-arm technology, more data is needed to optimize fluoroscopy protocols in accordance with as low as reasonably achievable (ALARA) principles. We investigated whether a “low-dose” (LD) protocol could reduce radiation exposure during fluoroscopy-guided access without compromising clinical outcomes.
Methods: Patients undergoing PCNL with fluoroscopy-guided percutaneous access at a tertiary care stone center between January 2019 to July 2021 were identified. A Philips Veradius C-arm was used. Prior to September 3, 2020, machine default settings were used: standard “per-frame” dose, 15 pulses per second (PPS) frame rate. After this date, a “low-dose” protocol was used which reduced the per-frame dose, reduced frame rate to 8 PPS for the needle puncture and used 4 PPS for the rest of the case. Demographic, imaging and clinical data (operative and fluoroscopy time, pre- and post-operative stone burden) were recorded. The primary outcome was cumulative radiation dose while secondary outcomes were stone-free status (SFS; defined as no fragments =2mm) and complications. Multivariate regression analysis was performed.
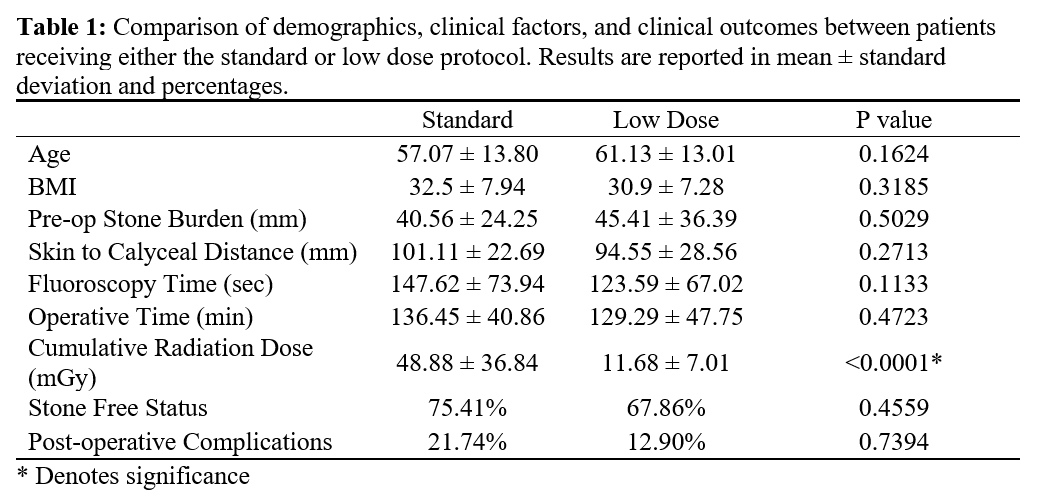
Results: One hundred patients were identified; 31 were in the LD group. The LD cohort had a significantly lower mean cumulative radiation dose of 11.68 mGy compared to 48.88 mGy (p < 0.0001). There were no differences in operative time, fluoroscopy time, stone burden, SFS or complications. In a regression model including skin-to-calyceal distance (STCD), stone burden, density, and location of access, higher STCD was associated with higher cumulative radiation dose. Higher preoperative stone burden was associated with longer operative time (p=0.0001) and lower odds of postoperative SFS (odds ratio=0.959, p=0.0007).
Conclusions: Use of “low-dose” pulsed fluoroscopy and decreased frame rate during PCNL drastically decreased radiation exposure four-fold without affecting stone-free status or complication rates. This technique adheres to ALARA principles and optimizes fluoroscopy technique without affecting the quality of the procedure.

.jpg)
.jpg)