Introduction: The learning curves for minimally invasive pyeloplasty techniques have been described in the past. However, the learning curve in achieving competency in open pyeloplasty has not been described. Hence, we aim to evaluate a single surgeon series of open pyeloplasty technique using the cumulative sum (CUSUM) methodology.
Methods: We retrospectively reviewed all open pyeloplasties performed by a single surgeon between January 2008 and March 2020. Collected variables included: sex, age at surgery, operative time, hospital stay, pre-operative ultrasound, pre-operative nuclear scans, pre-operative anteroposterior diameter, associated anomalies, laterality (left or right), type of stent, pre-operative split renal function, and duration of follow up. A CUSUM analysis was used: the highest peak, plateau and downward trends for complications (defined as Clavien-Dindo classification = 3) were identified on the plot and set as the transition points between five phases (learning, competency, proficiency, case-mix, and mastery).
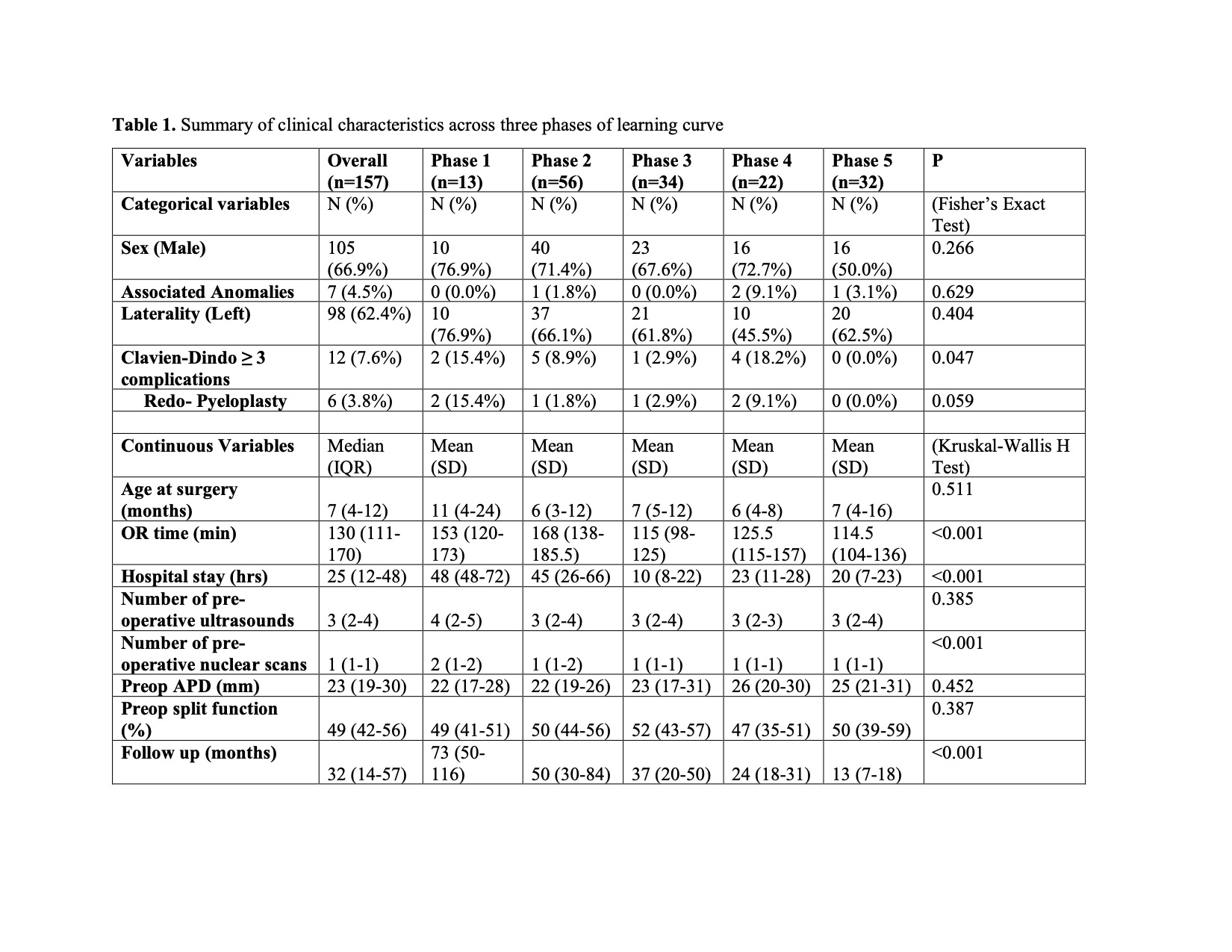
Results: Based on the CUSUM analysis, the index surgeon reached the competency phase after performing their 13th open pyeloplasty and became proficient after the 70th case. In the case-mix phase (104th to 126th cases), where the surgeon may be performing more complex cases while increasing trainee involvement, there was a slight increase in complication rates. After the 126th case, the surgeon entered the mastery phase, where there was consistent decreasing trend in complications (Table 1; Figure 1).
Conclusions: Surgeons performing open pyeloplasty in children following completion of their surgical training will continue to learn through their early cases until achieving competency. Technical competency may be reached after the 13th case.

.jpg)
.jpg)
 Kim, MD photo")