Introduction: Conservative management is now standard for most renal trauma as it decreases complications and nephrectomy rates. However, American Association for the Surgery of Trauma (AAST) grade V injuries renal injuries continue to largely require intervention and sparse data is available on conservative management. We investigate whether conservative management was pursued in patients who survive grade V renal injuries using the National Trauma Databank (NTDB).
Methods: Patients with grade V renal trauma were identified in the 2018 NTDB (n=612). Patients who survived to final hospital discharge were included (n=474). Conservative management was defined by the absence of any surgical or procedural intervention. Percutaneous or cystoscopic drain placement was exempted from procedural intervention. Characteristics of patients who underwent conservative vs non-conservative management were compared.
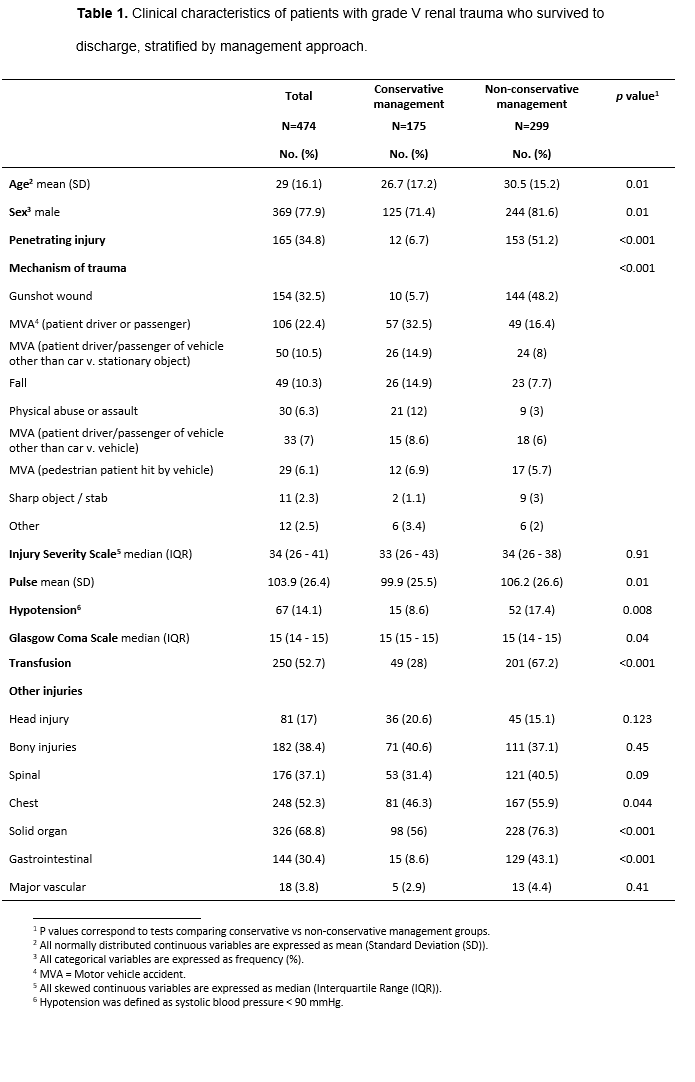
Results: Out of 474 patients, 175 (36.9%) were managed conservatively. In the 299 patients managed non-conservatively, most common interventions were surgical exploration (n=200, 66.9%), nephrectomy (n=196, 65.6%), kidney angioembolization (n=60, 20.1%), open surgical bleeding control (n=37, 12.4%), and surgical repair of the kidney or renal artery (n=22, 7.4%). Patient characteristics are depicted in Table 1, stratified by management approach. Patients managed conservatively had more favorable hemodynamic parameters compared to those managed non-conservatively, exhibiting lower mean pulse rate (99.9 vs 106.2, p=0.01). They had less hypotension on arrival (8.6% vs 17.4%, p=0.008) and received fewer blood transfusion (28% vs 67.2%, p<0.001). They also were younger (mean age 26.7 vs 30.5, p=0.01), less likely to be male (71.4% vs 91.6%, p=0.01), less likely to have sustained a penetrating injury (6.7% vs 51.2%, p<0.001), and had a significantly different distribution of trauma mechanism (Table 1).
Conclusions: A conservative approach may be safe in a subset of patients with grade V renal injury, especially in those who were less likely to be in shock, receive blood transfusion, or sustain penetrating injury. Further research to identify phenotypes amenable to conservative management is warranted to improve patient outcomes.

.jpg)
.jpg)