Introduction: Post-operative overprescribing of opioids contributes to the ongoing opioid epidemic. We evaluate the impact of statewide mandatory opioid stewardship initiatives (Prescription Drug Monitoring Plan verifications for prescriptions exceeding 3 days duration and opioid specific continuing medical education) implemented in 2017 on prescribing patterns following common urologic procedures.
Methods: We used Wisconsin Health Information Organization data, an all-payer claims database covering 75% of Wisconsin’s population, to identify patients undergoing stone (ureteroscopy, ESWL), endoscopic (TURP, TURBT) and major (prostatectomy, nephrectomy and cystectomy) surgeries statewide between January 1, 2016 and December 31, 2017. We captured filled opioid prescriptions within 7 days of a discharge and identified dose (median morphine milligram equivalents (MME)) and duration (median days) for the initial prescription. We compared prescribing between July and December 2016 to the same months in 2017 to allow for an appropriate wash-in period and control for seasonality.
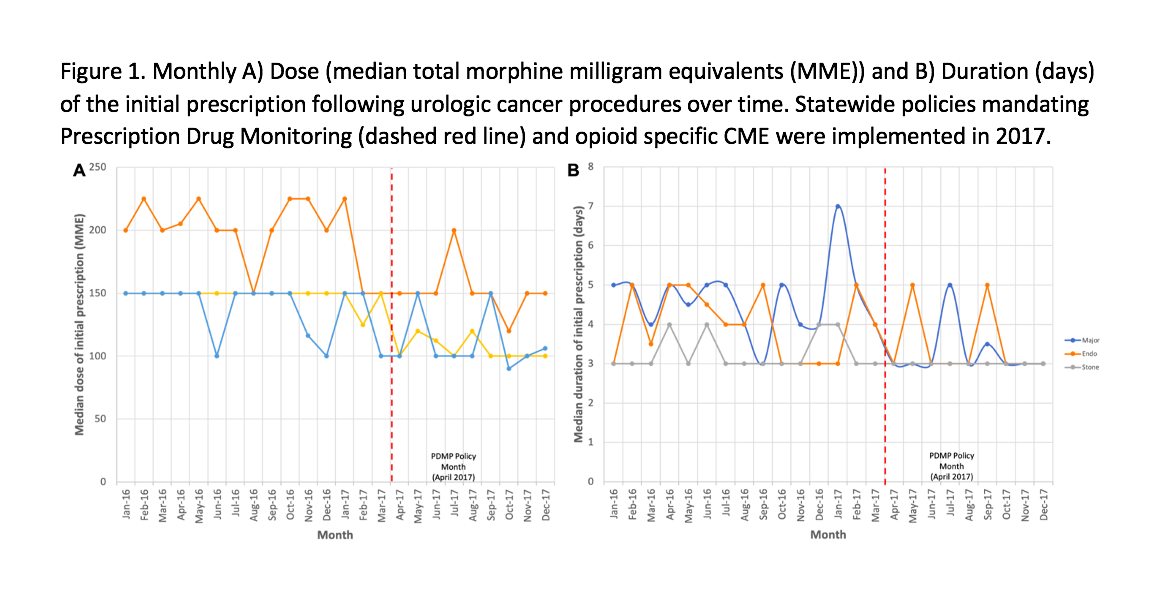
Results: We identified 3,788 patients (1,641 ureteroscopy, 581 ESWL, 600 TURP, 438 TURBT, 277 prostatectomy, 225 nephrectomy, and 26 cystectomy) undergoing our procedures of interest in the last 6 months of 2016 and 3,589 patients (1,498 ureteroscopy, 499 ESWL, 629 TURP, 400 TURBT, 312 prostatectomy, 231 nephrectomy, and 20 cystectomy) in the last six months of 2017. In 2016, prescriptions contained a median MME of 150 (IQR=100-150) and 4-day duration (IQR=3-4). In 2017, prescriptions contained a median MME of 112 (IQR=75-112.5) and 3-day duration (IQR=2-3. Median MME decreased for all procedure (p < 0.001) while prescription duration decreased from 4 to 3 days for major surgery (p < 0.001) and remained at 3 days for the other categories.
Conclusions: In Wisconsin, mandatory statewide opioid stewardship policies implemented in 2017 were associated with a decrease in prescription duration for major procedures but not endoscopic or stone procedures to comply with the policy. Modest changes in the dose prescribed occurred but prescribing remained in excess of guideline recommendations. Direct surgeon engagement and surgeon-led local initiatives may be better positioned to achieve continued improvements in opioid stewardship.

.jpg)
.jpg)