Introduction: Mixed reality (MR) allows the fusion of two video streams allowing real time overlay of a remote instructors hands onto the trainee’s view. We aim to evaluate remote MR training compared to in person (IP) training using a validated TRUS-Bx hydrogel simulation model.
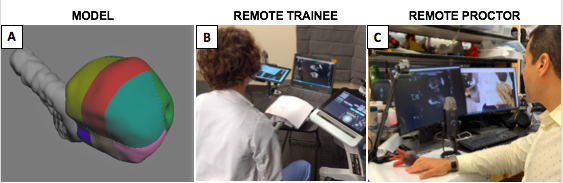
Methods: 14 participants with <5 case experience were randomized into MR and in person arms. All 14 reviewed educational videos of relevant anatomy and TRUS-BX steps followed by a pre-test, 3 training sessions, and post-test. During pre- and post-test participants independently measured the prostate, administered anesthetic and completed 14 biopsies on a validated hydrogel model with each biopsy area colored separately (Fig1A). Accuracy was defined as percentage of each core with the correct color corresponding to the biopsy area. During training sessions faculty guided trainees through procedural steps on a non-colored model either remotely using a MR platform or in person. MR set up included transmitting ultrasound view and audio via Zoom and displaying the merged surgical field with proctor hands on a tablet (Fig1B). The remote faculty annotated the ultrasound view and guided trainees with their hands using the merged surgical view (Fig1C). Post-training surveys evaluated trainee perceptions and proctor evaluations.
Results: On completion groups reported equal mean confidence in knowledge (MR: 80.6/100 vs IP: 87.8/100, p=0.49), ability to perform simulated TRUS (89.8 vs 90, p=0.97) and live TRUS (66.8 vs 71, p=0.73) . Pre-test core percentage was similar among groups (MR: 17.9% vs IP: 26.4%, p=0.44). Both groups experienced significant increases in post-test scores (75.9% for MR and 62.3% for IP groups). MR groups increase was x1.5 times greater (MR: +58.0% vs IP: +35.9%, p<0.01) despite trainee perceptions that remote training may hinder their ability to learn. Faculty rated the trainee skills from 1 (below expectations) to 3 (exceeds expectations) for TRUS manipulation, gland measurement, anesthetic, and biopsy. The MR group averaged 0.5, 0.1, 0.8 and 0.5 higher respectively.
Conclusions: Remote training using MR technology provided equivalent learning to in-person simulation training. This technology has the potential for cross-institutional training.

.jpg)
.jpg)