Introduction: Several groups have reported using a hybrid room for percutaneous nephrolithotomy (PCNL). We report the results of a series of elective PCNL cases performed in our facility’s hybrid room employing a robotic biplane fluoroscopy system (Artis Zeego, Siemens), with regard to effective radiation dose (ERD). Our null hypothesis was that PCNL using the Hybrid system (H-PCNL) would have the same ERD for standard fluoroscopy (excluding advanced imaging techniques), as traditional PCNL (T-PCNL).
Methods: All PCNL cases performed at our VA facility between 2014 to present were reviewed. Mean ERD was calculated by converting dose area product (DAP) using a published conversion factor of 0.25 mSv/Gy*cm2 (Compagnone). Our practice has transitioned to H-PCNL using ultrasound-guided percutaneous access (with only secondary use of fluoroscopy). Therefore, the comparison group was defined as cases with percutaneous access by Interventional Radiology (IR) prior to T-PCNL (n=15). Mean ERDs were compared using a two-way t-test.
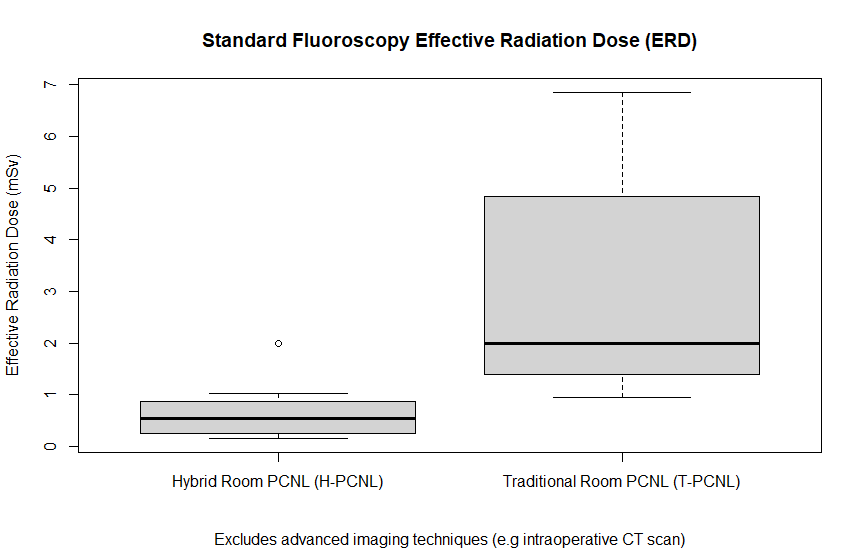
Results: Eight H-PCNL cases (seven patients), each involving a new percutaneous access by the urologist, were performed at our facility since March 2021. 29 first-stage T-PCNL cases were performed since 2014 by the same surgeons. The mean intraoperative ERD for H-PCNL cases was 0.69 mSv (median 0.54), compared to 3.03 mSv (median 2.0) for T-PCNL with prior IR access (p=0.001). As anticipated, mean ERD was higher at 3.70 mSv (median 3.0) for T-PCNL with concurrent urologist access (n=14). Hybrid room imaging quality was considerably better with a much larger field of view. Mean stone size was 4.2 cm (median 2.9) in the H-PCNL group vs. 3.4 cm (median 3.2) with T-PCNL. BMI (28.51 vs. 26.34), age (70.5 vs. 64), and ASA-4 status (29% vs 6.7%) were higher with H-PCNL. 7/8 (87.5%) of H-PCNL cases were supine, while 14/15 (93.3%) of T-PCNL cases were prone.
Conclusions: ERD of standard fluoroscopy was 77% lower with H-PCNL cases than T-PCNL, despite patients in the traditional group having similar stone size and lower BMI. Apart from the benefits of advanced imaging capabilities of a hybrid room system (e.g. intraoperative 3D imaging), lower radiation doses to patients and clinicians is a compelling reason to transition to H-PCNL to improve safety.

.jpg)
.jpg)