MP50: Kidney Cancer: Localized: Surgical Therapy III
MP50-02: How important are morphologic subtypes on the prognosis of surgically treated non-metastatic papillary renal cell carcinoma? An analysis from a contemporary multi-institutional database
Urologic Oncology Division of Urology Department, Istanbul University Istanbul Faculty of Medicine
Introduction: Papillary renal cell carcinoma (papRCC) is currently divided in 2 morphologic subtypes: type 1 and type 2. The aim of this contemporary multi-institutional study is to investigate the role of morphologic subtypes on the prognosis of surgically treated non-metastatic papRCC.
Methods: This study was conducted using a multi-institutional database consisting of 1219 patients with histopathologically confirmed non-metastatic papRCC after partial or radical nephrectomy collected from 8 tertiary European insitutions. The patients with accurate data for morphologic subtypes (type 1 and type 2) and follow-up records were included into this study. Clinical and histopathological parameters, recurrence free survival (RFS), cancer specific survival (CSS) and overall survival (OS) were compared between subtypes. Chi-square and Mann-Whitney U tests, and Kaplan-Meier survival analysis were used for the comparisons. Multivariable Cox Regression analysis was used to assess independent predictors on survival outcomes.
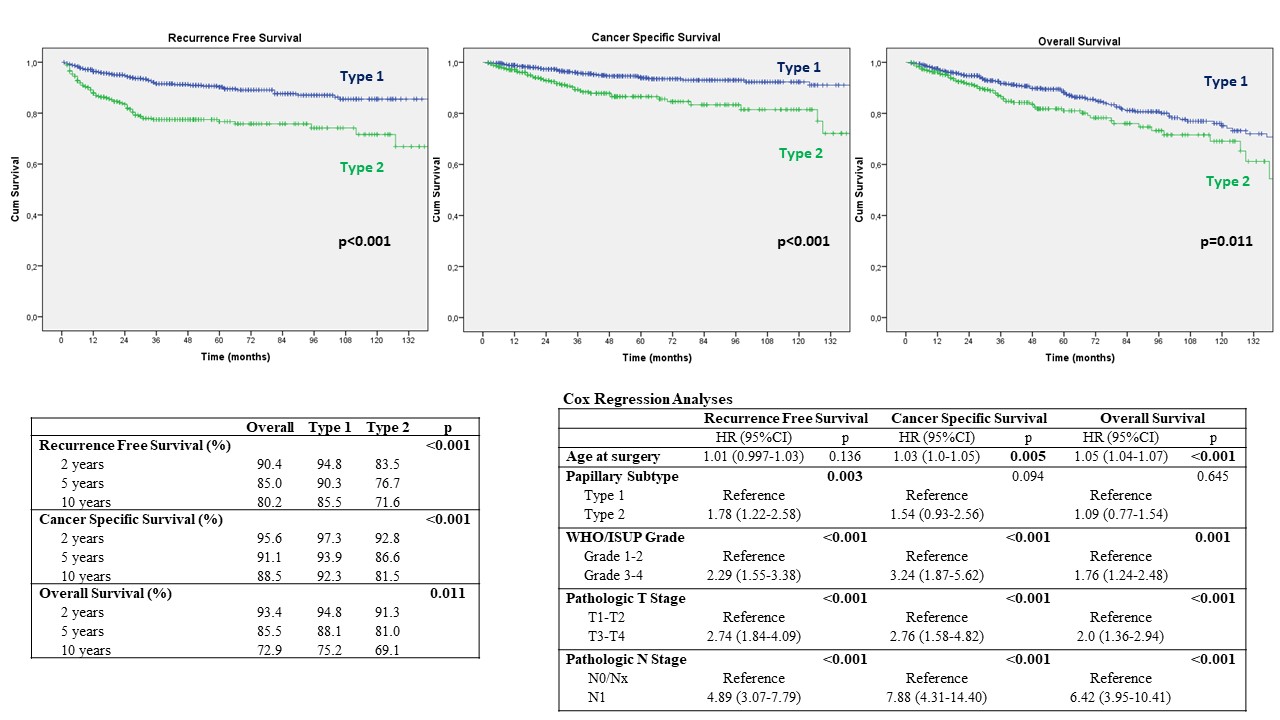
Results: A total of 879 patients were identified for this study. The patients in the type 2 group were older (64 vs. 66 years, p=0.006), had greater tumor size (3.8 vs. 4.3 cm, p=0.01) and more frequently underwent radical nephrectomy (25.7 vs. 35.2%, p=0.002). Nuclear grade (p < 0.001), pathologic T stage (p < 0.001) and N stage (p < 0.001) were significantly higher in the type 2 group. The median follow-up was 48 (IQR:24-88) months. Kaplan-Meier survival analyses showed that 5 year RFS (90.3% vs. 76.7%, p<0.001), CSS (93.9% vs. 86.6%, p<0.001) and OS (88.1% vs. 81.0%, p=0.011) were significantly lower in type 2 papRCC. Age, grade, pathologic T and N stage adjusted Cox-Regression analyses found that type 2 was independent predictor for RFS (HR:1.78 [95%CI:1.22-2.58], p=0.003), but not for CSS (HR:1.54 [95%CI:0.93-2.56], p=0.094) and OS (HR:1.09 [95%CI:0.77-1.54], p=0.645)
Conclusions: This contemporary multi-institutional study with a large dataset suggested that type 2 was associated with adverse histopathological outcomes, and was an independent predictor of RFS after surgical treatment of non-metastatic papRCC. These findings may guide decision making on follow-up schedule after surgery, and risk stratification for the adjuvant trials, in the individualized medicine era.

.jpg)
.jpg)