University at Buffalo Jacobs School of Medicine and Biomedical Sciences
Introduction: Renal cell carcinoma (RCC) is treated with a planned surgery of the affected kidney. We aimed to investigate the risk factors that may necessitate an emergency nephrectomy for RCC.
Methods: Clinical and demographic information were extracted from National Surgical Quality Improvement Program (NSQIP) database for patients who underwent nephrectomy from 2005-2017. Univariate and multivariate analyses were used to assess the independent factors contributing to an emergency nephrectomy. We also analyzed the role of emergency nephrectomy in postoperative adverse events and mortality through univariate analyses. P values less than 0.05 were considered significant.
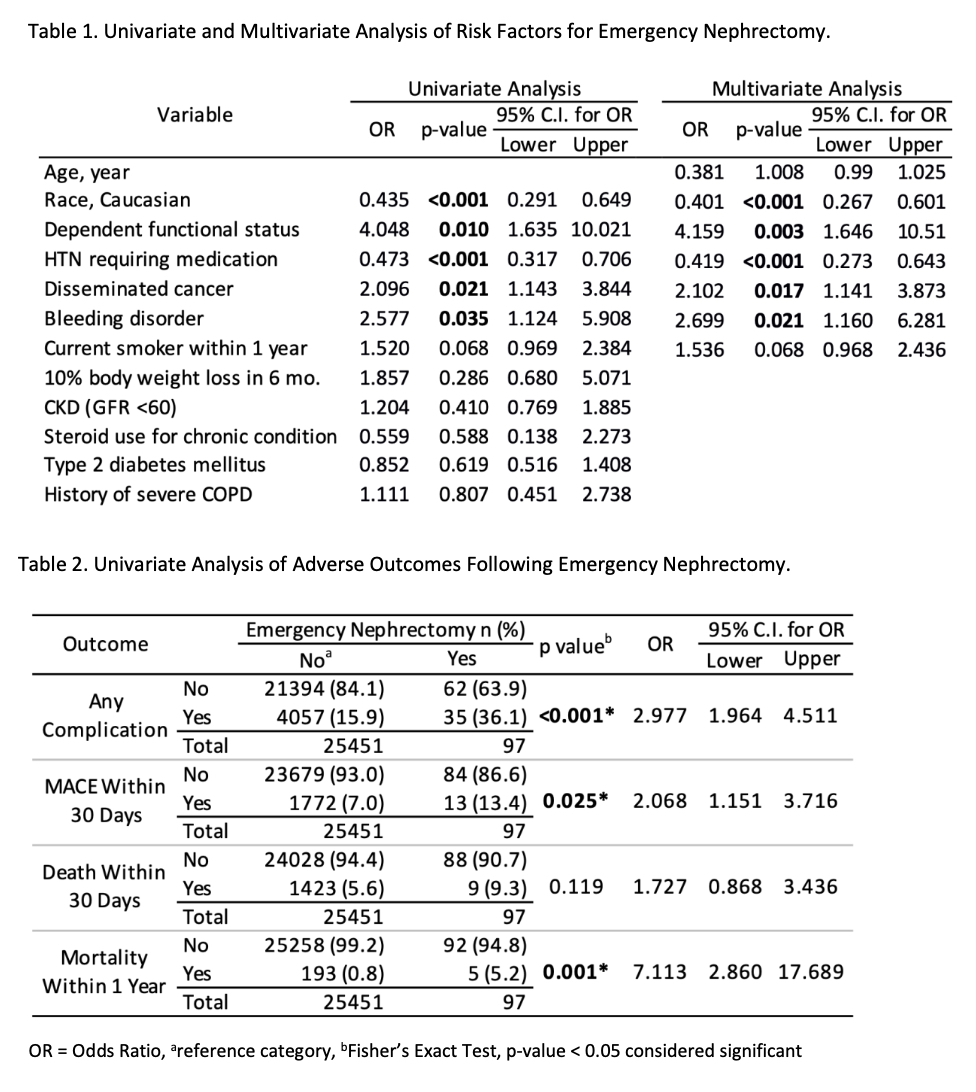
Results: From 25,548 patients who underwent nephrectomy for RCC from 2005 through 2017, emergency nephrectomy was performed in 97 patients (0.4%). Compared to elective nephrectomy, emergent nephrectomy was associated with preoperative “dependent” status (OR=4.05 [CI: 1.64-10.02], p<0.01), disseminated cancer (OR=2.10 [CI: 1.14-3.84], p=0.021), and bleeding tendency(OR=2.58 [CI: 1.12-5.91], p=0.035). Caucasian race and hypertension were protective against emergency nephrectomy (OR=0.44 [CI: 0.29-0.65], p<0.001 and OR=0.47 [CI: 0.32-0.71], p<0.001, respectively). Following multivariable analysis, preoperative “dependent” status increased the risk of emergency nephrectomy 4-fold (OR=4.16 [CI: 1.65-10.51], p=0.003) while hypertension decreased the risk of emergency nephrectomy by half (OR=0.42 [CI: 0.27-0.64], p<0.001). Compared to elective nephrectomy, emergency nephrectomy was associated with increased risk of early post-operative complication (OR=2.98 [CI: 1.96-4.51], p<0.001) and major adverse cardiac events (OR=2.07 [CI: 1.15-3.72], p=0.025), and hospital mortality (OR=7.11 [CI: 2.86-17.69], p=0.001).
Conclusions: RCC patients undergoing emergency nephrectomy are more likely to have disseminated cancer, bleeding disorders, and preoperative dependent status. Dependent functional status is a major independent risk factor for emergency nephrectomy, while hypertension is protective against emergency nephrectomy. Practitioners must be aware of factors increasing the risk of emergency nephrectomy for RCC, leading to a higher occurrence of post-surgical adverse events and hospital mortality.

.jpg)
.jpg)