MP52: Urodynamics/Lower Urinary Tract Dysfunction/Female Pelvic Medicine: Male Incontinence: Therapy
MP52-13: Presenting Signs and Symptoms of Artificial Urinary Sphincter Cuff Erosion
Monday, May 16, 2022
7:00 AM – 8:15 AM
Location: Room 228
Linley Diao*, Samantha Nealon, Shervin Badkhshan, Avery Wolfe, Gianpaolo Carpinito, Benjamin Dropkin, Sarah Sanders, Steven Hudak, Allen Morey, Dallas, TX
Introduction: Presenting signs and symptoms of artificial urinary sphincter (AUS) cuff erosion are not well established in the urological literature. We sought to characterize the most common presentation and clinical risk factors for erosion to distinguish the relative frequency of symptoms that should trigger further evaluation in these unfortunate patients.
Methods: We retrospectively reviewed our large tertiary center database to identify men who presented with cuff erosion between 2007 and 2020. A similar cohort of men who underwent AUS placement without erosion were randomly selected from the same database for comparison. Risk factors for cuff erosion – pelvic radiation, androgen deprivation therapy (ADT), high-grade prostate cancer (Gleason score = 8) – were recorded for each patient. Presenting signs and symptoms of erosion were grouped into three categories: obstructive symptoms, worsening incontinence, and localized scrotal inflammation (SI).
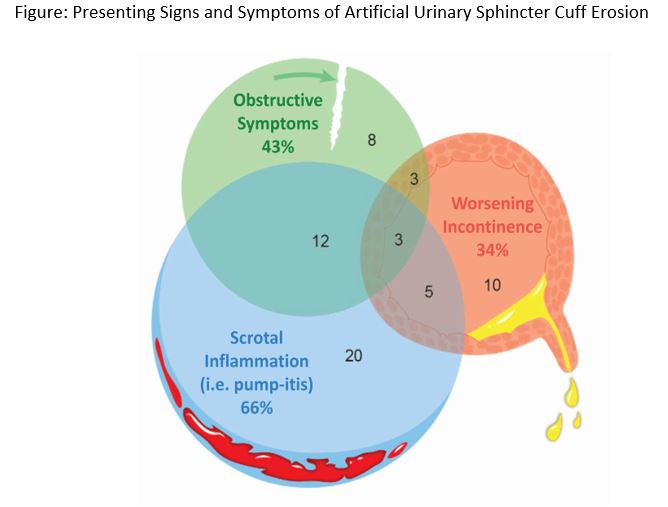
Results: Of 893 men who underwent AUS placement during the study interval, 61 (6.8%) sustained cuff erosion. Most erosion patients (40/61, 66%) presented with scrotal inflammatory changes including tenderness, erythema, and swelling (Figure 1). Fewer men reported obstructive symptoms (26/61, 43%) and worsening incontinence (21/61, 34%). The average length of time to cuff erosion was 22.2 months ± 33.7. Men with SI or obstructive symptoms presented significantly earlier than those with worsening incontinence (SI 14 ± 18 vs. obstructive symptoms 15 ± 16 vs. incontinence 37 ± 48 months after AUS insertion, p<0.01). Relative to the non-erosion control group (n=61), men who suffered erosion had a higher prevalence of pelvic radiation (71 vs 49%, p=0.02), hypertension (87 vs 64%, p=0.003), coronary artery disease (54 vs 12 %, p<0.00001), and smoking history (71 vs 51%, p=0.03).
Conclusions: AUS cuff erosion most commonly presents as scrotal inflammatory symptoms. Obstructive voiding symptoms and worsening incontinence are also common. Any of these symptoms should prompt further investigation of cuff erosion.

.jpg)
.jpg)