Introduction: Urinary incontinence after prostate cancer therapy can significantly affect quality of life, with some men eligible for corrective surgery. Our objective is to evaluate the potential racial disparities for surgical management of urinary incontinence in patients who have undergone prior prostate cancer therapy.
Methods: Medicare claims from 2004-2013 were used to identify men aged 66 years or older who met inclusion criteria and underwent either prostatectomy (RP) or radiation (RT). Medicare Part A and B claims for incontinence were captured using HCPCS and ICD-9-CM codes along with the associated codes for the therapeutic surgeries. Differences in the covariates between treatment groups were evaluated using pairwise Chi-Square tests, and time to event analyses for surgery were calculated using Kruskal-Wallis tests. Outcomes were reported as hazard ratios with 95% confidence intervals, with statistical significance being reported as p < 0.05 on SASTM.
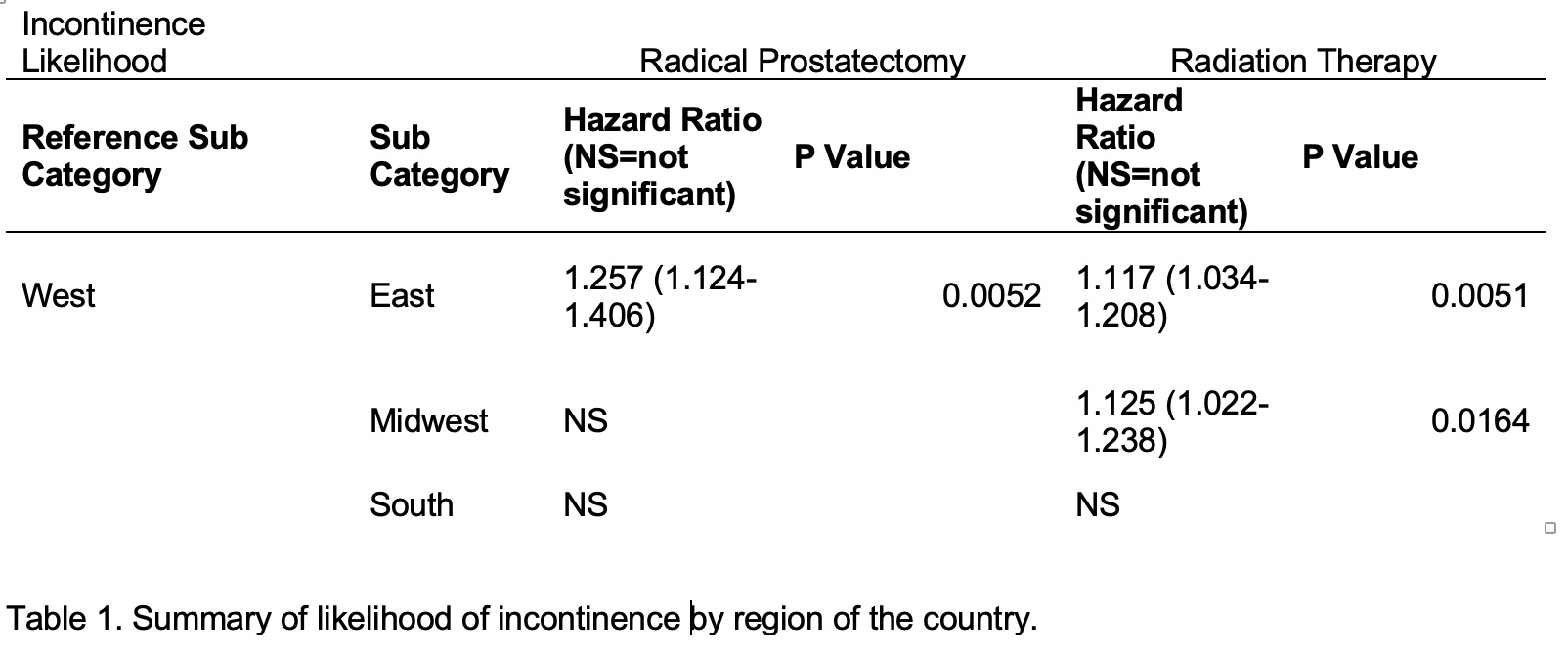
Results: A total of 63,158 men were identified in the cohort of which 15,143 men underwent RP and 44,694 underwent RT. There was no statistically significant difference in rates of incontinence surgery such as artificial urinary sphincter (AUS) and male sling (MS) between white and black men after either RT or RP. Black men had delayed treatment for incontinence compared to white men (27 vs 25 months for AUS and 27.5 vs 22 months for male sling). Men in the east were more likely to have incontinence after both RP and RT compared to men in the west but were not more likely to have any corrective surgery for this (Table 1). Men from the south were not more likely to have incontinence after RP compared to men from the west, but were more likely to get a MS (1.356 (1.086-1.692), p <0.0071).
Conclusions: There was no difference in overall rates of surgical treatment for incontinence after either RT or RP between white and black men. There was a difference between men in the east vs west. These results may help improve counseling for men eligible for incontinence surgery, including based on region of the country but not stratified by race. Future research is needed in identifying the systems that may be associated with delayed surgical care.

.jpg)
.jpg)