MP56-13: Role of radical cystectomy and lymph node dissection in patients with non-metastatic clinically advanced lymph nodal (cN2/N3) bladder cancer: An analysis from National Cancer Database
Monday, May 16, 2022
10:30 AM – 11:45 AM
Location: Room 228
HARSHIT GARG*, FURKAN DURSUN, Ahmed Elshabrawy, Hanzhang Wang, MICHAEL LISS, DHARAM KAUSHIK, ROBERT SVATEK, Ahmed Mansour, SAN ANTONIO, TX
Introduction: The role of radical cystectomy in non-metastatic clinically advanced lymph nodal (cN2/N3) bladder cancer is controversial. This study aims to compare the outcomes of patients undergoing radical cystectomy (RC) vs systemic therapy only in patients with non-metastatic bladder cancer with clinical N2/N3 disease.
Methods: We queried the National Cancer Database for patients with non-metastatic muscle-invasive bladder cancer (cT2-T4N2-3M0), who presented with advanced lymphadenopathy. Patients were classified as Group A: Those who received definitive surgery with or without neoadjuvant/ adjuvant therapy, Group B: Those who received systemic therapy alone and Group C: Those who did not receive any treatment. The predictive factors for undergoing definitive surgery were identified using multivariate regression analysis. Inverse probability propensity weighting was utilized to balance groups. The overall survival (OS) was evaluated using Kaplan Meir survival analysis and predictors for survival were studied using multivariate cox regression analysis.
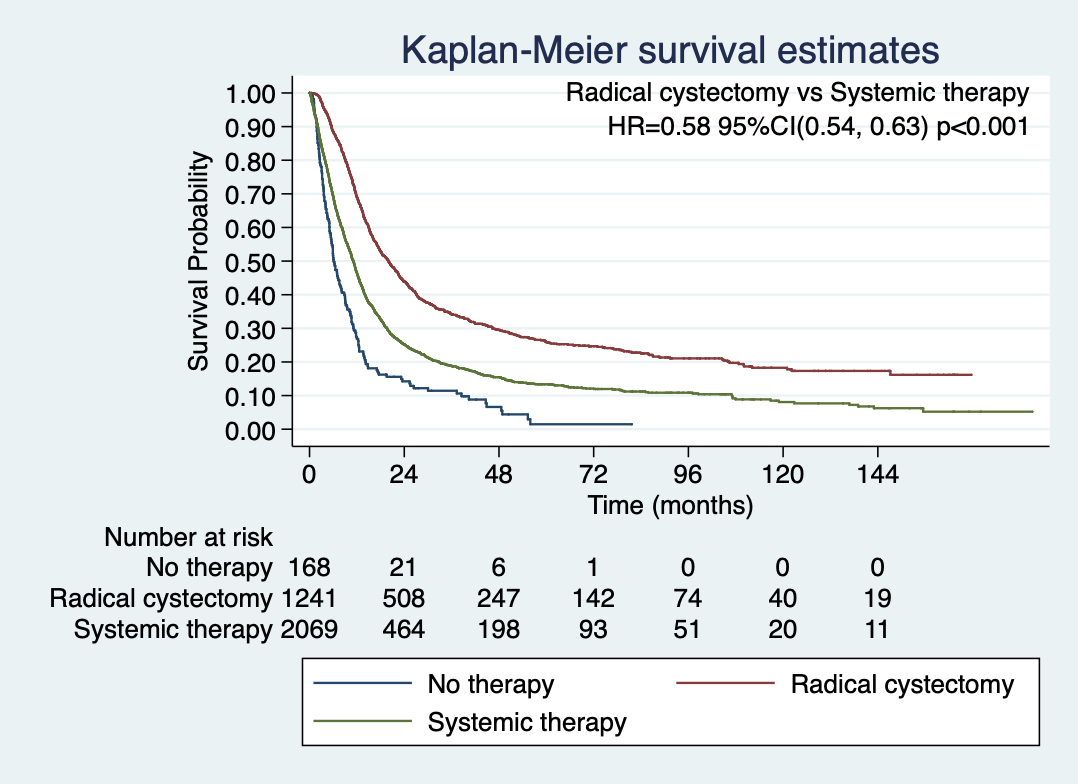
Results: A total of 2,725 patients were identified and classified into Group A (n=1,366), Group B (n=2,372) and Group C (n=190). The predictive factors for undergoing RC were male gender (OR= 1.16, p=0.05), age below 70 years (OR=1.36, p=0.006), white race compared to black race (OR=1.38, p=0.009) and histology of micropapillary urothelial carcinoma (OR=2.37, p=0.004). The median (IQR) overall survival was 20 (10.5-66.8) months in Group A, 11.1(4.9-24.2) months in Group B and 6.1(3.2-12.4) months in Group C (p < 0.001).13.2 (IQR). After weighted analysis, patients undergoing radical cystectomy had significantly higher 5-year OS as compared to systemic therapy group [25.9% vs 13.4%, p<0.001] [Figure 1]. Radical cystectomy was identified as an independent predictor for overall survival (compared to systemic therapy) [HR=0.58, p<0.001]
Conclusions: In clinically advanced non-metastatic lymph nodal disease (T2-T4,N2/N3) of bladder cancer, radical cystectomy offers superior survival benefit compared to systemic therapy.

.jpg)
.jpg)