Associate Researcher Roswell Park Comprehensive Cancer Center
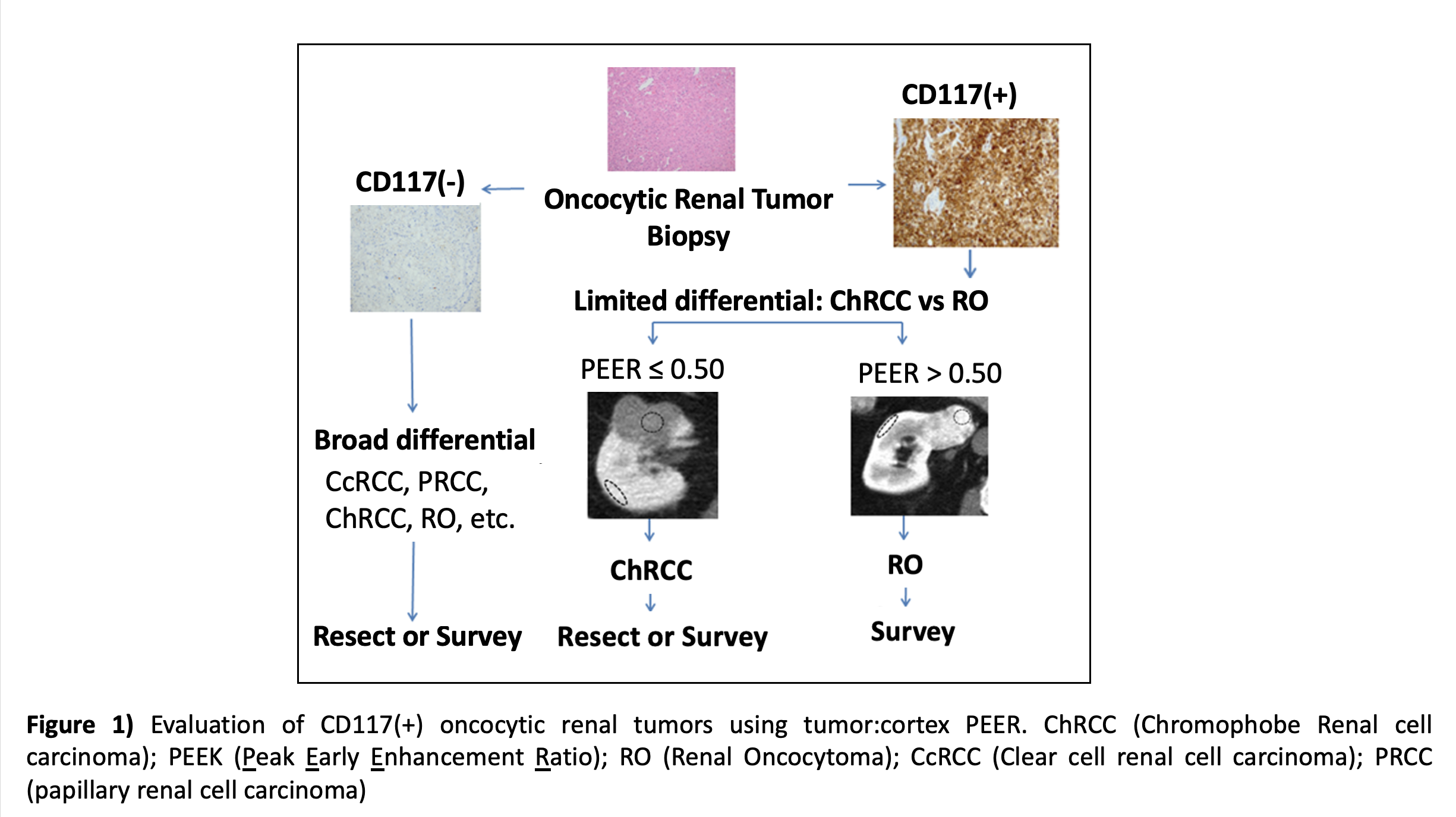
Introduction: The tumor:cortex peak early-phase enhancement ratio (PEER) on CT images has been prospectively validated for differentiating CD117(+) benign renal oncocytoma (RO) from histologically similar CD117(+) chromophobe renal cell carcinoma (ChRCC), including outperformance of the CK7 ChRCC biomarker. We describe our 8.5-year experience using routine renal mass biopsy (RMB) with CD117 immunostain and tumor:cortex PEER score to avoid RO resection.
Methods: From January 2013 to July 2021, all oncocytic RMB patients managed by a single urologist at a National Comprehensive Cancer Network institute underwent prospective CD117 and CK7 immunostaining followed by radiographic tumor:cortex PEER scoring of CD117(+) cases. All CD117(+) patients with a PEER score supporting RO diagnosis (score >0.55) were recommended active surveillance (AS). Resection was considered for PEER score <0.55 or CD117(-) staining. All clinically localized renal cortical tumor (RCT) patients seen by this urologist over the 8.5 year period were retrospectively reviewed to determine 1) rate of pathological RO resection, and 2) CD117(+) RO AS outcomes.
Results: 238 RCT patients underwent immediate or delayed resection over 8.5 years, during which 299 RCT patients underwent AS/observation only. Most (309/537, 57%) patients had an RMB of which 64 (20.4%) were oncocytic (43 RO, 13 ChRCC and 8 other RCC), including 52 CD117(+) cases (40 favored RO, 12 chRCC). All RO CD117(+) patients were corroborated by PEER scoring (median score 0.79, range 0.56-1.14) and managed with AS. All 238 RCT resections had final pathology of RCC (n=237) or necrotic fat-poor AML of indeterminate malignant potential (n=1), with no (0/238, 0%) RO resections. All patients (40/40, 100%) with CD117(+) RO supported by PEER remain on AS without symptoms, >cT3 upstaging or metastasis after median follow up of 43 months.
Conclusions: Combined use of routine RMB, CD117 immunostaining and PEER scoring is an effective diagnostic approach to safely avoid CD117(+) RO resection. Here we report the first large nephrectomy patient series to our knowledge with complete avoidance of RO resection. Allowing for occasional diagnostic resection of >cT2 and CD117(-) RO variants, an RO resection rate of ~2% should be a feasible new standard of care.

.jpg)
.jpg)