Kidney Cancer: Epidemiology & Evaluation/Staging/Surveillance II
PD18-02: External validation of the ASSURE model to predict oncological outcomes after resection of high-risk renal cell carcinomas
Saturday, May 14, 2022
7:10 AM – 7:20 AM
Location: Room 255
Zine-Eddine Khene*, Rennes, France, Alessandro Larcher, Milan, Italy, Jean-Christophe BERNHARD, Bordeaux, France, Nicolas Doumerc, Toulouse, France, Romain BOISSIER, Marseille, France, Idir Ouzaid, Paris, France, Philippe BARTHELEMY, Strasbourg, France, Morgan Roupret, Paris, France, Francesco MONTORSI, Milan, Italy, Pierre Bigot, Angers, France, Karim Bensalah, Rennes, France
Introduction: A prognostic model based on the population of the ASSURE phase III trial has recently been described. The ASSURE model stratifies patients into risk groups to predict survival after surgical resection of intermediate and high-risk localized kidney cancer. Our objective was to validate the ASSURE model in a large independent multi-institutional cohort of patients treated in a “real life” setting outside of a clinical trial.
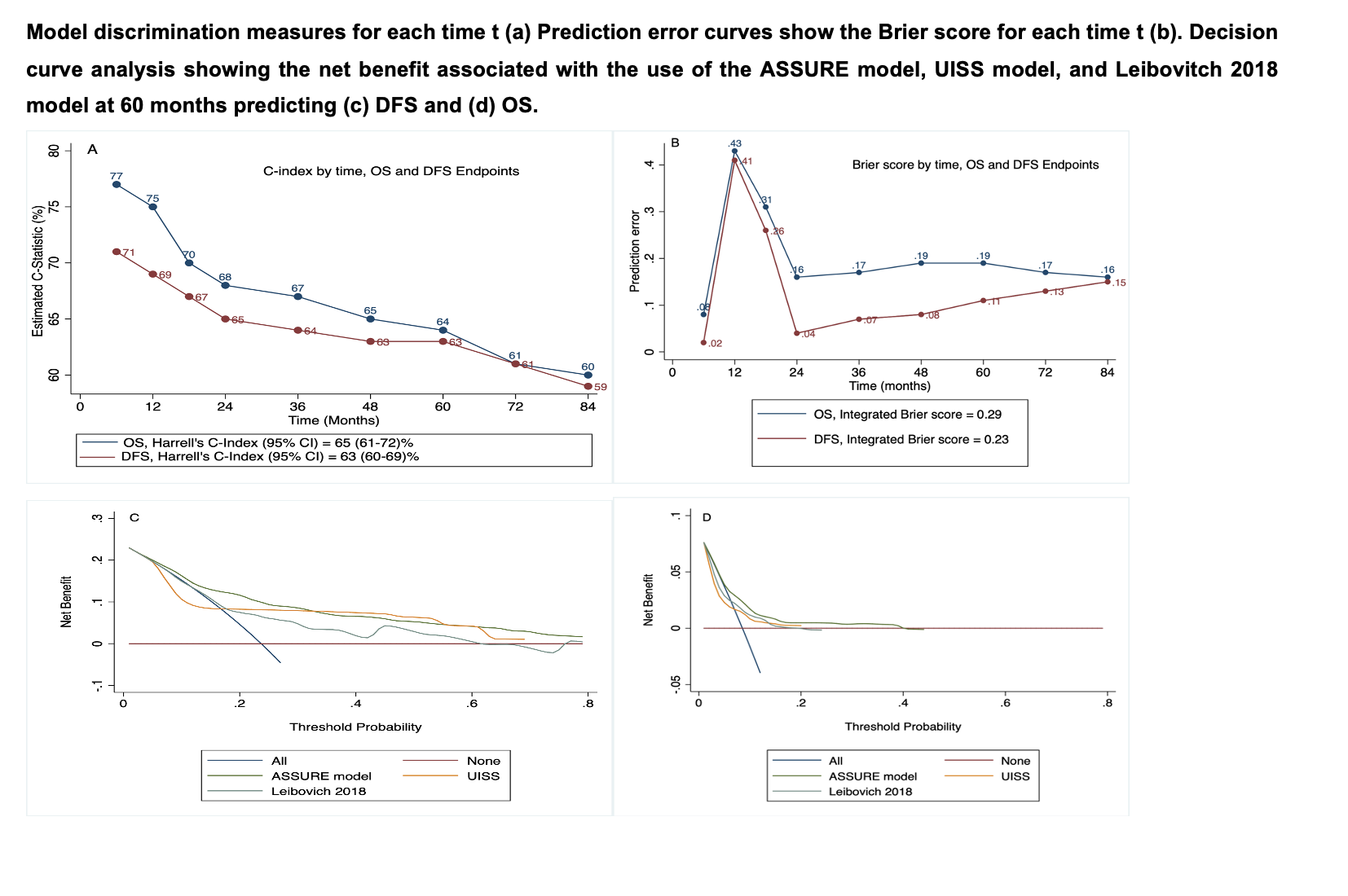
Methods: Data of patients from ten institutions who underwent radical or partial nephrectomy for a non-metastatic RCC between 2013 and 2019 were analyzed. We exclusively focused on patients with pT1b and ISUP 3-4, pT2, pT3, pT4, and N1 (i.e., those classified as intermediate and high risk according to the ASSURE model). The performance of the ASSURE model was evaluated in terms of discrimination and calibration. In addition, decision curve analysis (DCA) was used to determine whether the clinical value of the new model increased the net benefit over a realistic range of threshold probabilities. Finally, DCA of the ASSURE model was compared with that of older UCLA Integrated Staging System (UISS) and Leibovich 2018 score.
Results: 1372 patients were included in the analysis. Median age was 64 years (IQR 55-72). Median tumor size was 6.5 cm (IQR 5-9). The majority of tumors were clear cell RCCs (77%), of high ISUP grade (72% of grade 3 and 4), with 45% exhibiting tumor necrosis and 5% harboring nodal involvement. Median follow up was 54 months (IQR 32-75). Regarding disease-free survival, the ASSURE model showed modest discrimination (65%), miscalibration and poor net benefit compared with UCLA Integrated Staging System (UISS) and Leibovich 2018 models. Similarly, the ability of the ASSURE model to predict overall survival was poor in terms of discrimination (63%), with an overestimation on calibration plots and a modest net benefit for probability threshold between 10-40%.
Conclusions: The ASSURE model is the last reported prognostic model that evaluates survival after surgical resection of a non-metastatic renal cell carcinoma. An improvement of patient classification was not clearly established when compared with available models, and implementation of this model in this setting still needs to be clarified.

.jpg)
.jpg)